
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-126
Unforeseen Consequences, But Expected Outcome - A Complicated TASH Case
By Wan Faizal Wan Rahimi Shah, Rosli Mohd Ali, David Soon Ping Chew
Presenter
Wan Faizal Wan Rahimi Shah
Authors
Wan Faizal Wan Rahimi Shah1, Rosli Mohd Ali2, David Soon Ping Chew3
Affiliation
Cardiac Vascular Sentral Kuala Lumpur (CVSKL), Malaysia1, Cardiac Vascular Sentral Kuala Lumpur, Malaysia2, National Heart Institute, Malaysia3,
View Study Report
TCTAP C-126
Coronary - Complication Management
Unforeseen Consequences, But Expected Outcome - A Complicated TASH Case
Wan Faizal Wan Rahimi Shah1, Rosli Mohd Ali2, David Soon Ping Chew3
Cardiac Vascular Sentral Kuala Lumpur (CVSKL), Malaysia1, Cardiac Vascular Sentral Kuala Lumpur, Malaysia2, National Heart Institute, Malaysia3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
61 years old female came for opinion. She was diagnosed with Hypertrophic Cardiomyopathy before. However as she was asymptomatic, she was not under regular follow up. This episode, she has been suffering from exertional dyspnea, which is impeding her daily activities. She recalled having prescribed Beta blocker and Calcium Channel Blocker before, but could not tolerate it due to her borderline low blood pressures.

Relevant Test Results Prior to Catheterization
Echo revealed concentric LVH (IVSd 2.1 cm) with good systolic function. No obvious RWMA seen. Biplane LVEF is 73%. However SAM + with LVOT obstuction was noted. Mild Mitral & Tricuspid Regurgitation were observed. Measurements of gradients are as below -
After multi-disciplinary discussion, patient opted for Trans-coronary Ablation of Septal Hypertrophy.
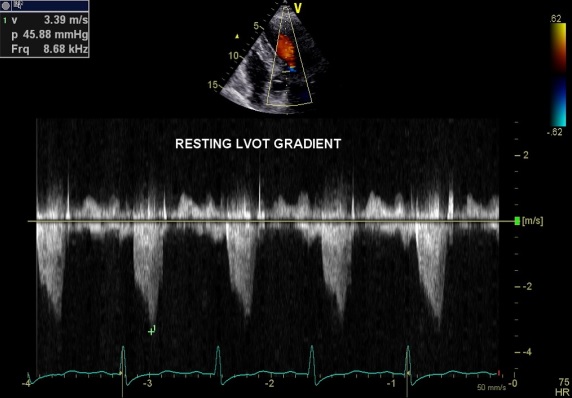
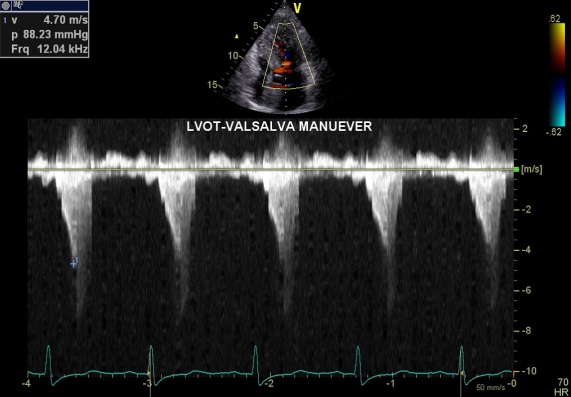
| Resting | Valsalva | |
| Basal (LVOT) | 69 mmHg | 89 mmHg |
| Mid | 43 mmHg | 55 mmHg |
| Apical | 26 mmHg | 31 mmHg |
After multi-disciplinary discussion, patient opted for Trans-coronary Ablation of Septal Hypertrophy.
Relevant Catheterization Findings
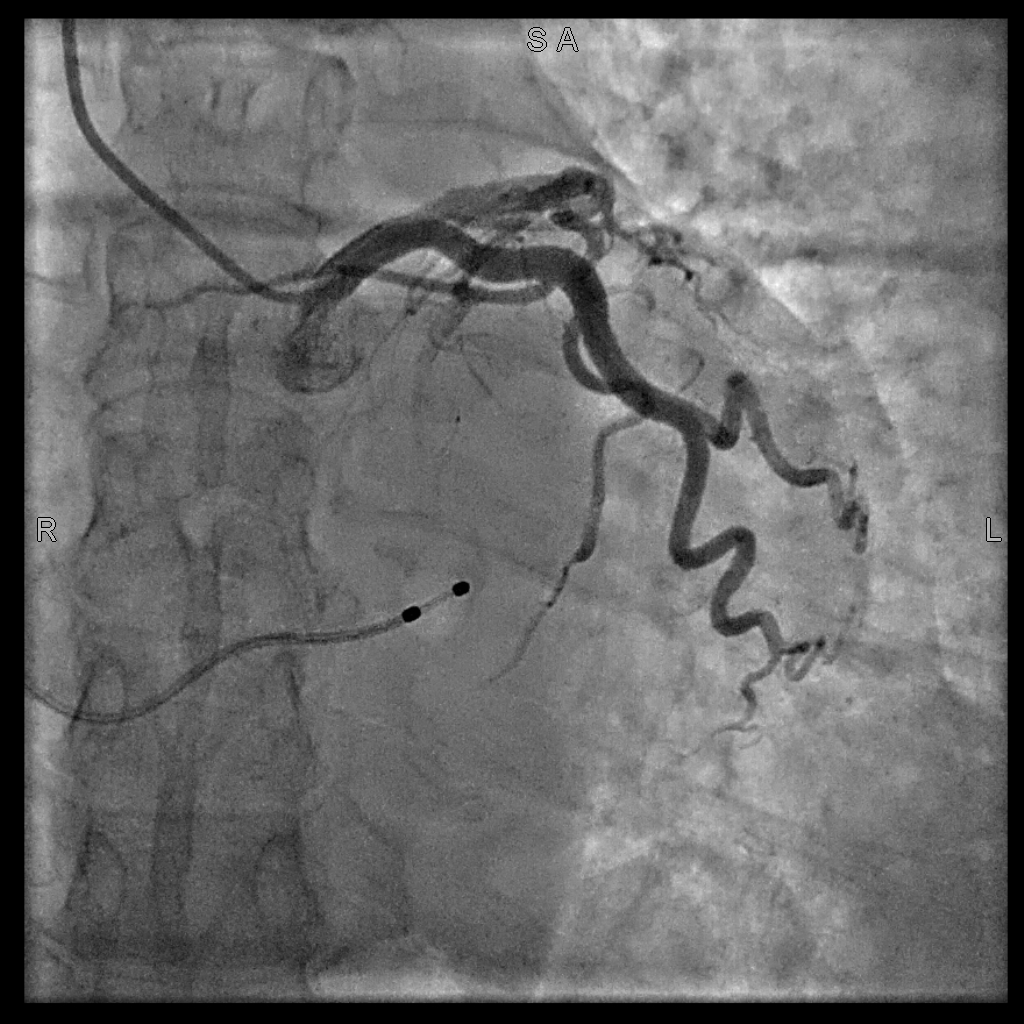
Right radial access was obtained. Coronary Angiogram revealed relatively normal coronaries. 2nd septal branch was observed to be suitable target for alcohol injection. A 7Fr Mach 1 CLS 3.5 was utilized, but subsequently downgraded to 3.0 for better engagement. Before proceeding, a temporary pacing wire was inserted via right internal jugular vein.

Interventional Management
Procedural Step
There were lack of OTW balloons with short lengths available in our centre. An OTW Jade 2.0 x 20 mm balloon with RT floppy guidewire was wired with difficulty. After inflation at 6 atm, myocardial area supplied was identified with contrast injection and Echo. No backflow into LAD ensured. 1 ml alcohol injected. Planned for 2nd injection, but unable to rewire through (likely compromised lumen due to angle of septal branch). Used Grand Slam wire with extension but still failed to rewire. Decided to remove balloon and use another new one.
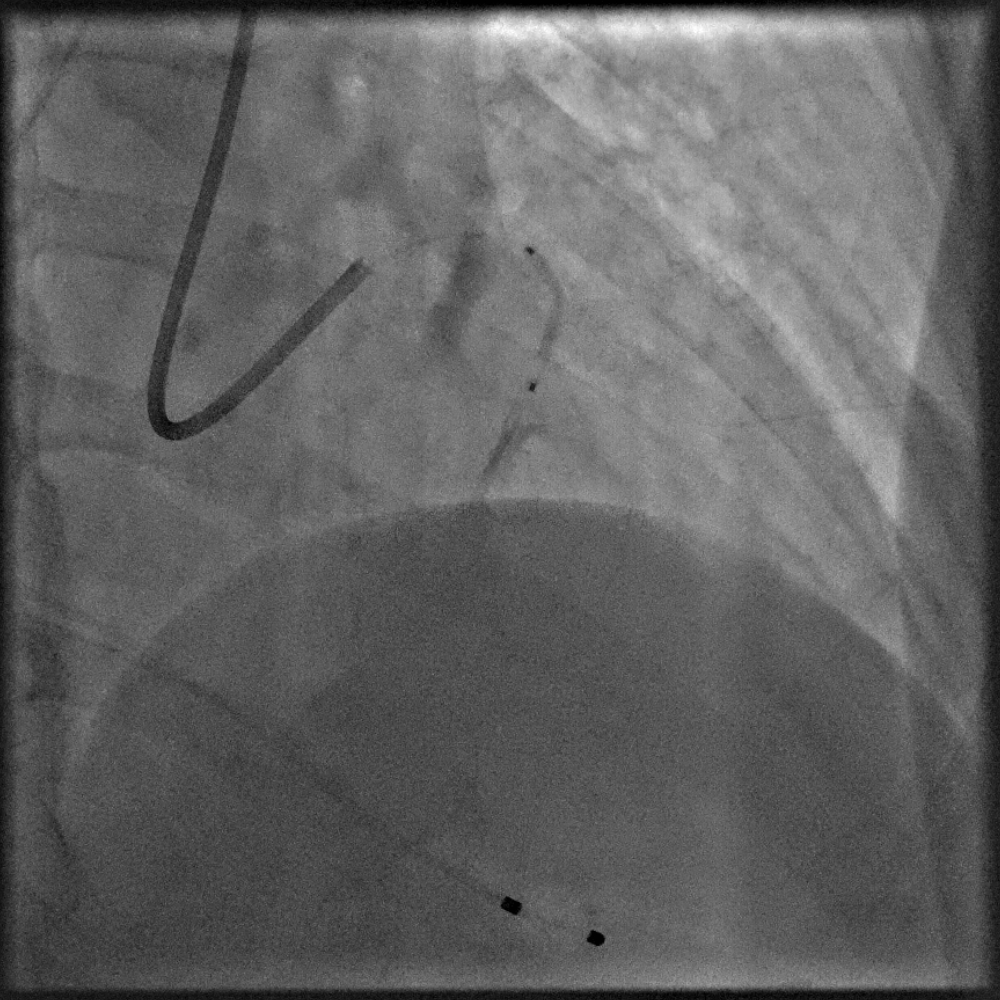
Another OTW Sprinter 1.5 x 15 mm used. However after inflation and contrast injection, noted septal perforation. Progressive retrograde flow of contrast seen from septal into LAD & D2 with narrowing of both lumen. Rewired septal branch with Finecross microcatheter and 2 Tornado coils inserted. No more flow down branch observed. However in view of persistent contrast staining in LAD, decided for IVUS interrogation.
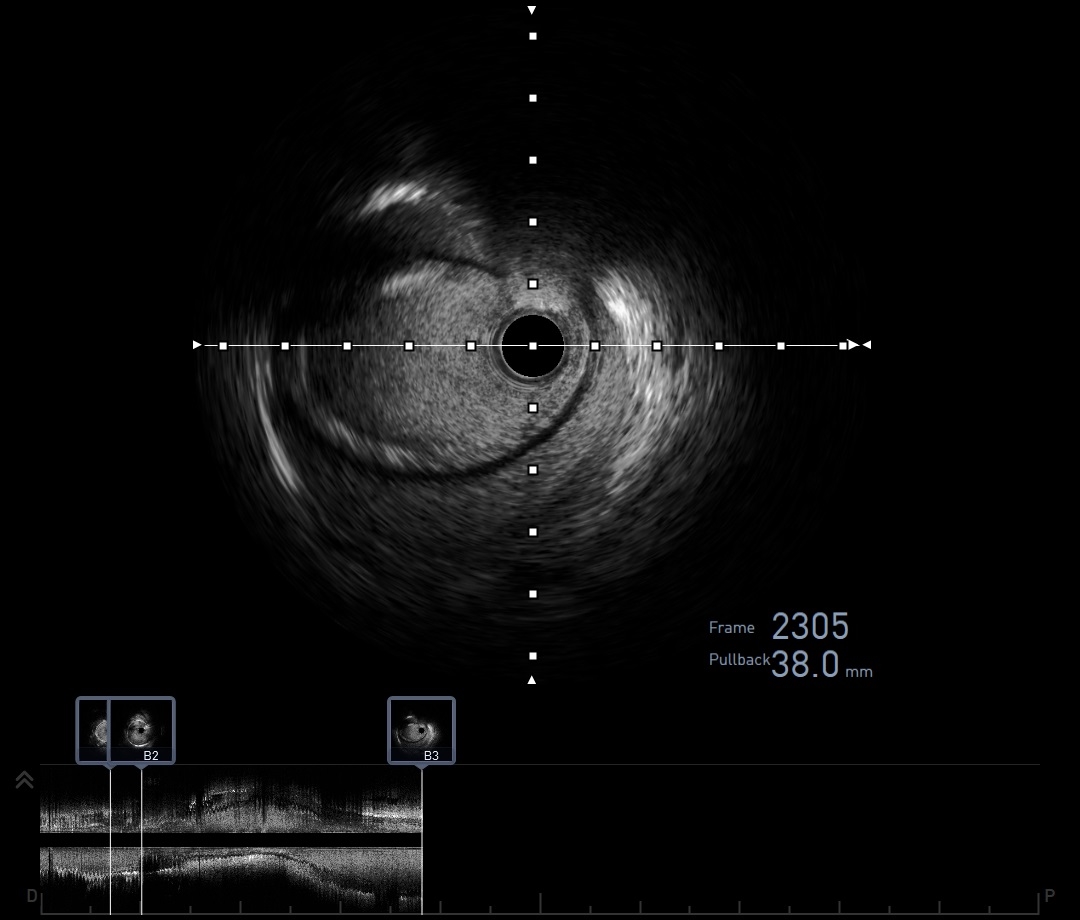
IVUS of both LAD and D2 showed contained hematoma. LMS and LCx were not affected. Interestingly, no breakage of intima at any point area where hematoma was observed. Decision made to leave hematoma alone for spontaneous resolution.
Patient remained hemodynamically stable throughout. TIMI III flow seen down all left system vessels. Echo post TASH down showed peak gradient across LVOT dropped to 43 mmHg with mild hypokinesia in basal septum.

Another OTW Sprinter 1.5 x 15 mm used. However after inflation and contrast injection, noted septal perforation. Progressive retrograde flow of contrast seen from septal into LAD & D2 with narrowing of both lumen. Rewired septal branch with Finecross microcatheter and 2 Tornado coils inserted. No more flow down branch observed. However in view of persistent contrast staining in LAD, decided for IVUS interrogation.
IVUS of both LAD and D2 showed contained hematoma. LMS and LCx were not affected. Interestingly, no breakage of intima at any point area where hematoma was observed. Decision made to leave hematoma alone for spontaneous resolution.
Patient remained hemodynamically stable throughout. TIMI III flow seen down all left system vessels. Echo post TASH down showed peak gradient across LVOT dropped to 43 mmHg with mild hypokinesia in basal septum.
Case Summary
This case depicts an immediate septal perforation, resulting in retrograde hematoma formation in LAD and D2 branch. Source of perforation was secured with coils. We were fortunate that patient's vessels were normal and could contain the hematoma, without another intima tear elsewhere and without compromising lumen integrity.
Although the mechanism was unclear, we postulated the cause as being acute angle of septal branch coupled with long balloon jutting out into the LAD. This probably created a shearing effect in the fragile septal branch at the balloon shoulder.
In the end, a successful infarction of the basal septum was achieved by coils and not alcohol as what the procedure intended.
Although the mechanism was unclear, we postulated the cause as being acute angle of septal branch coupled with long balloon jutting out into the LAD. This probably created a shearing effect in the fragile septal branch at the balloon shoulder.
In the end, a successful infarction of the basal septum was achieved by coils and not alcohol as what the procedure intended.