
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-060
The Anchor-Balloon Technique for Difficult Chronic Total Occlusions
By Pitchayathinan Jiratchayachote
Presenter
Pitchayathinan Jiratchayachote
Authors
Pitchayathinan Jiratchayachote1
Affiliation
Pranangklao Hospital, Thailand1,
View Study Report
TCTAP C-060
Coronary - Complex PCI - CTO
The Anchor-Balloon Technique for Difficult Chronic Total Occlusions
Pitchayathinan Jiratchayachote1
Pranangklao Hospital, Thailand1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
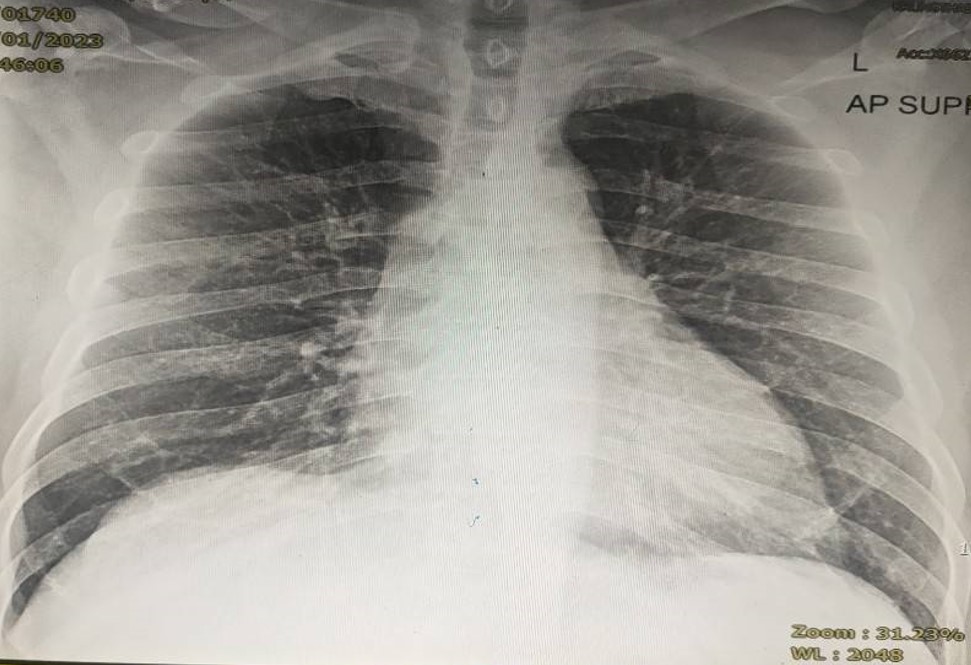
A 65-year-old male with type 2 diabetes, hypertension, and dyslipidemia presented to the emergency department with chest pain radiating to the left shoulder. Examination indicated a blood pressure of 154/90 mmHg, a regular heart rate of 105 bpm, and symmetrical breath sounds without adventitious sounds in the respiratory system. A cardiovascular examination revealed a normal S1S2 pattern with no murmurs.
Relevant Test Results Prior to Catheterization
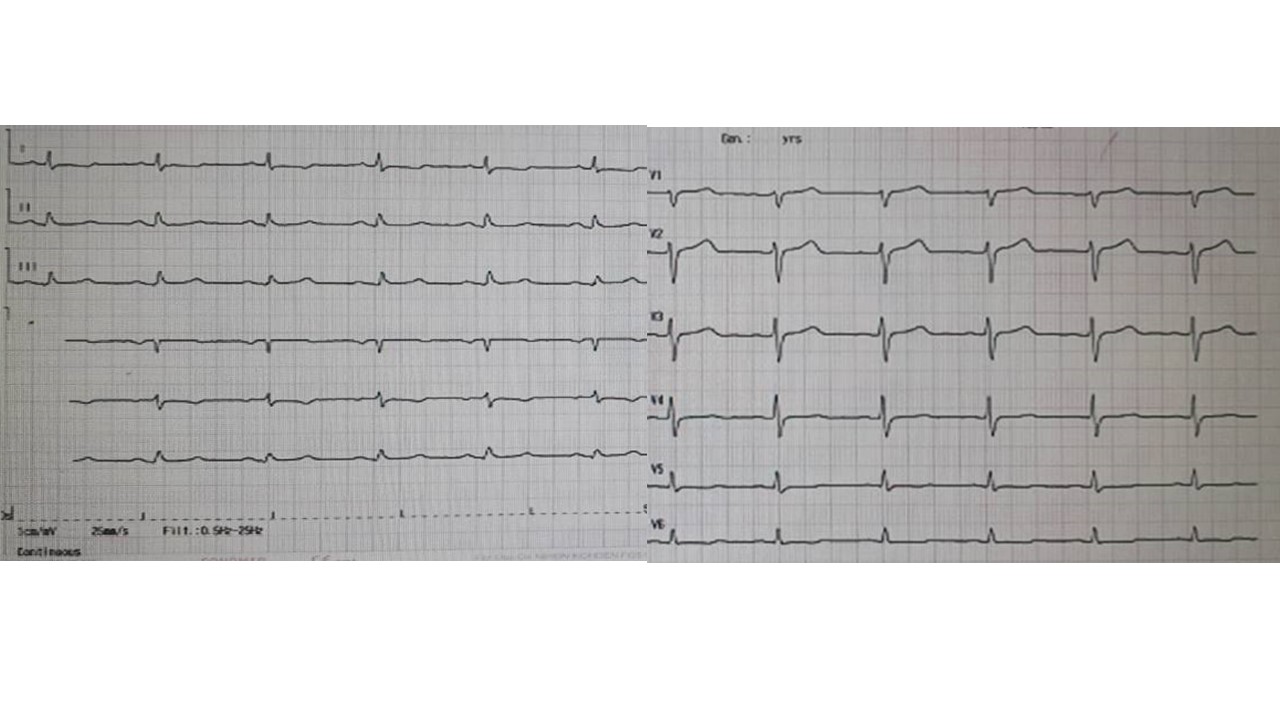
EKG showed normal sinus rhythm at 71 bpm. with Q wave at II, III, aVFThe echocardiogram showed LV hypertrophy, good LV systolic function, LVEF 54%, inferior wall hypokinesia, and mild MR. Mild TRTroponin I 1592 ng/ml
Relevant Catheterization Findings
Right dominant coronary artery systemLM: no significant stenosisLAD: no significant stenosis, give collateral to RCALCx: 60% stenosis at proximal LCx, subtotal occlusion at OM1, CTO at OM2RCA: Diffused disease, 70% stenosis at proximal RCA, 80% stenosis at mid-RCA, CTO distal RCA
Interventional Management
Procedural Step
Initial Attempt:Right femoral access with a 6 Fr sheath engaged the RCA through a JR4/6Fr catheter. Fielder XT and Finecross microcatheter adeptly traversed the CTO RCA. Attempts with a 1.0x6mm SC balloon failed, leading to guide catheter disengagement. The Sion wire was then employed. Pre-dilation of proximal and mid-RCA stenosis utilized a 2.0 x 15 mm SC balloon, followed by deploying 2.5 x 18 mm SES and 2.75 x 12 mm SES at the mid-proximal RCA, both at 12 atm. The final angiogram revealed a subtotal occlusion in the distal RCA.
Second Attempt:Right femoral access was obtained using 7 Fr sheath. AL-1 short tip/7Fr and JR4.0/7Fr cannot engage to RCA. A 6Fr/JR3.5 guide catheter effectively engaged the RCA. Employing the anchor balloon strategy, the RV branch was wired with Sion. Rinato, guided by Finecross, advanced to the distal RCA. A 2.0 x 15mm SC balloon in the RV branch expanded to a nominal pressure of 8 atm, providing stable support. This facilitated the smooth advancement of the 1.0x6mm SC balloon through the subtotal occlusion at 16 atm. Subsequent interventions deployed SC balloons 1.5 x 10mm, 2.0 x 15mm, and 3.0 x 15mm at 16 atm. In the distal RCA, a meticulously placed 3.0 x 40mm SES at 11 atm was followed by post-dilatation, using a 3.0 x 15mm NC balloon for the distal RCA at 12 atm and a 3.5 x 15 mm NC balloon for the proximal-mid RCA at 12 atm.

 CHANTHET_NAPAT_(S9_F1-1).avi_snapshot_00.00_[2023.11.17_19.57.11].jpg
CHANTHET_NAPAT_(S9_F1-1).avi_snapshot_00.00_[2023.11.17_19.57.11].jpg


CHANTHET_NAPAT_(S85_F1-33).avi_snapshot_00.01_[2023.11.17_20.01.13].jpg
Second Attempt:Right femoral access was obtained using 7 Fr sheath. AL-1 short tip/7Fr and JR4.0/7Fr cannot engage to RCA. A 6Fr/JR3.5 guide catheter effectively engaged the RCA. Employing the anchor balloon strategy, the RV branch was wired with Sion. Rinato, guided by Finecross, advanced to the distal RCA. A 2.0 x 15mm SC balloon in the RV branch expanded to a nominal pressure of 8 atm, providing stable support. This facilitated the smooth advancement of the 1.0x6mm SC balloon through the subtotal occlusion at 16 atm. Subsequent interventions deployed SC balloons 1.5 x 10mm, 2.0 x 15mm, and 3.0 x 15mm at 16 atm. In the distal RCA, a meticulously placed 3.0 x 40mm SES at 11 atm was followed by post-dilatation, using a 3.0 x 15mm NC balloon for the distal RCA at 12 atm and a 3.5 x 15 mm NC balloon for the proximal-mid RCA at 12 atm.
Case Summary
In summary:1. Adequate guide catheter support is crucial for uncrossing balloons in CTO lesions2. Strategies include using a larger guide catheter with a more supportive shape, long arterial sheaths, deep engagement, guide catheter extension, anchor wire, buddy wire, and anchor balloon in strategic locations like the side branch, distal target vessel, or subintimal areas below the lesion. 3. In this case, a nearly perpendicular take-off and total occlusion of the distal RCA, using an anchoring balloon in the RV branch is a prudent alternative to optimize guiding catheter support. 4. Caution is necessary to prevent unintended damage to the side branch during balloon anchoring.