
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-077
A Challenging Case of Complicated CTO Revascularization With Life-Threatening Cardiac Tamponade
By Yu-Lan Liu, Yen-Lien Chou
Presenter
Yu-Lan Liu
Authors
Yu-Lan Liu1, Yen-Lien Chou1
Affiliation
Tri-Service General Hospital, Taiwan1,
View Study Report
TCTAP C-077
Coronary - Complex PCI - CTO
A Challenging Case of Complicated CTO Revascularization With Life-Threatening Cardiac Tamponade
Yu-Lan Liu1, Yen-Lien Chou1
Tri-Service General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
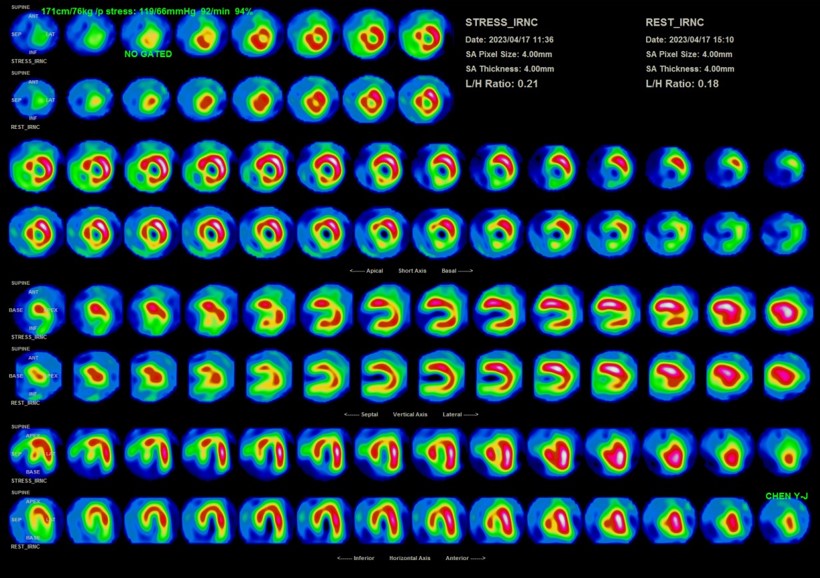
An 82-year-old man with hypertension, chronic obstructive pulmonary disease, and stage 4 chronic kidney disease was admitted to ICU due to pneumonia with acute respiratory failure post endotracheal intubation and mechanical ventilation. He presented with marked bradycardia and persistent pleural effusion during training program for weaning ventilator. Thallium-201 MPI showed myocardial ischemia at 30% of anterior wall and 15% of inferior wall. Hence, the cardiac catheterization was performed.

Relevant Test Results Prior to Catheterization
Hemoglobin: 7.6 g/dLPlatelet: 62 10^3/uLProthrombin time: 17.0 secondsInternational normalized ratio: 1.2Blood urea nitrogen: 57 mg/dLCreatine: 2.8 mg/dLC-reactive protein: 2.6 mg/dLN-terminal pro-brain natriuretic peptide (NT-Pro-BNP): 12396 pg/mL
Relevant Catheterization Findings
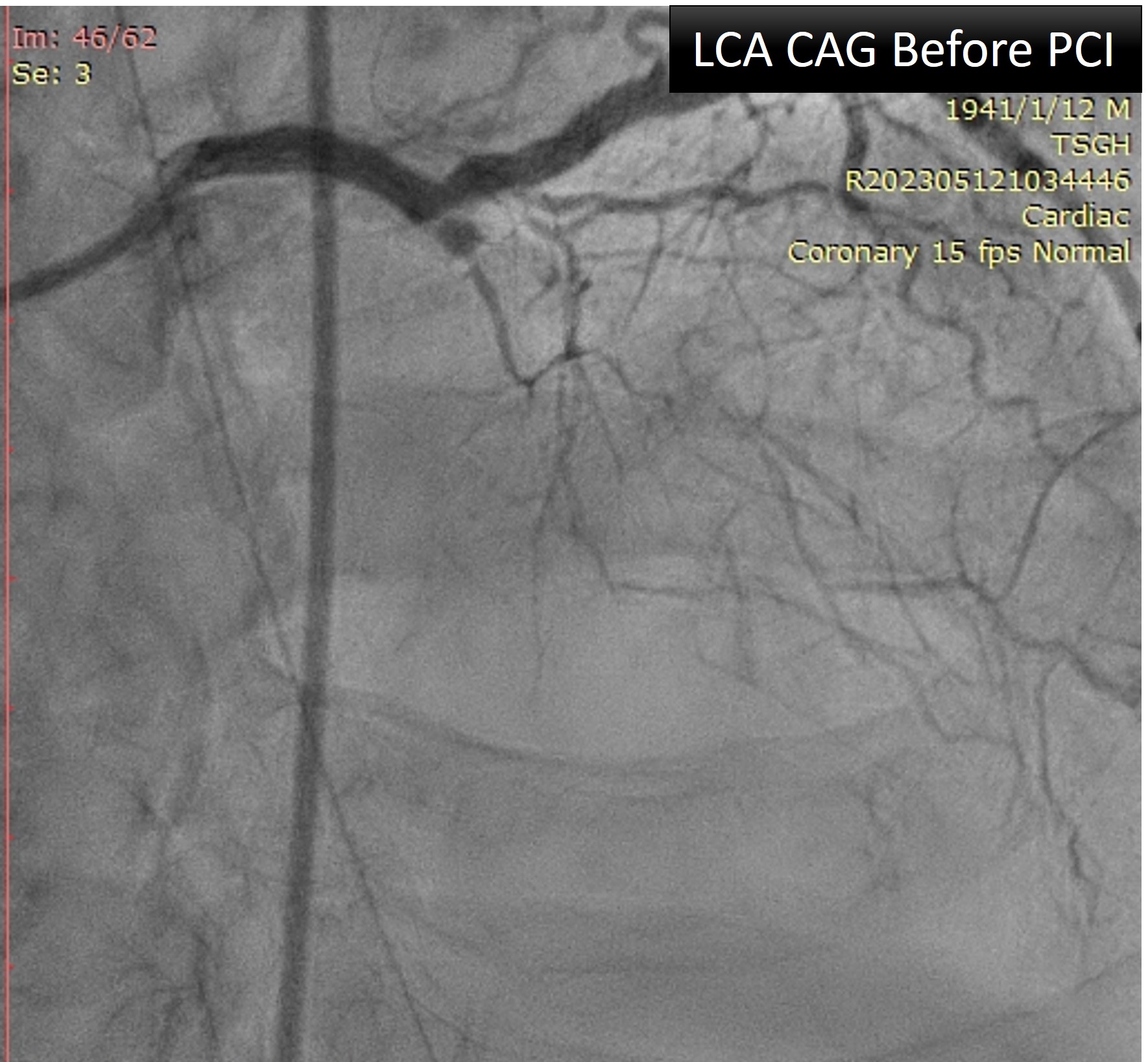
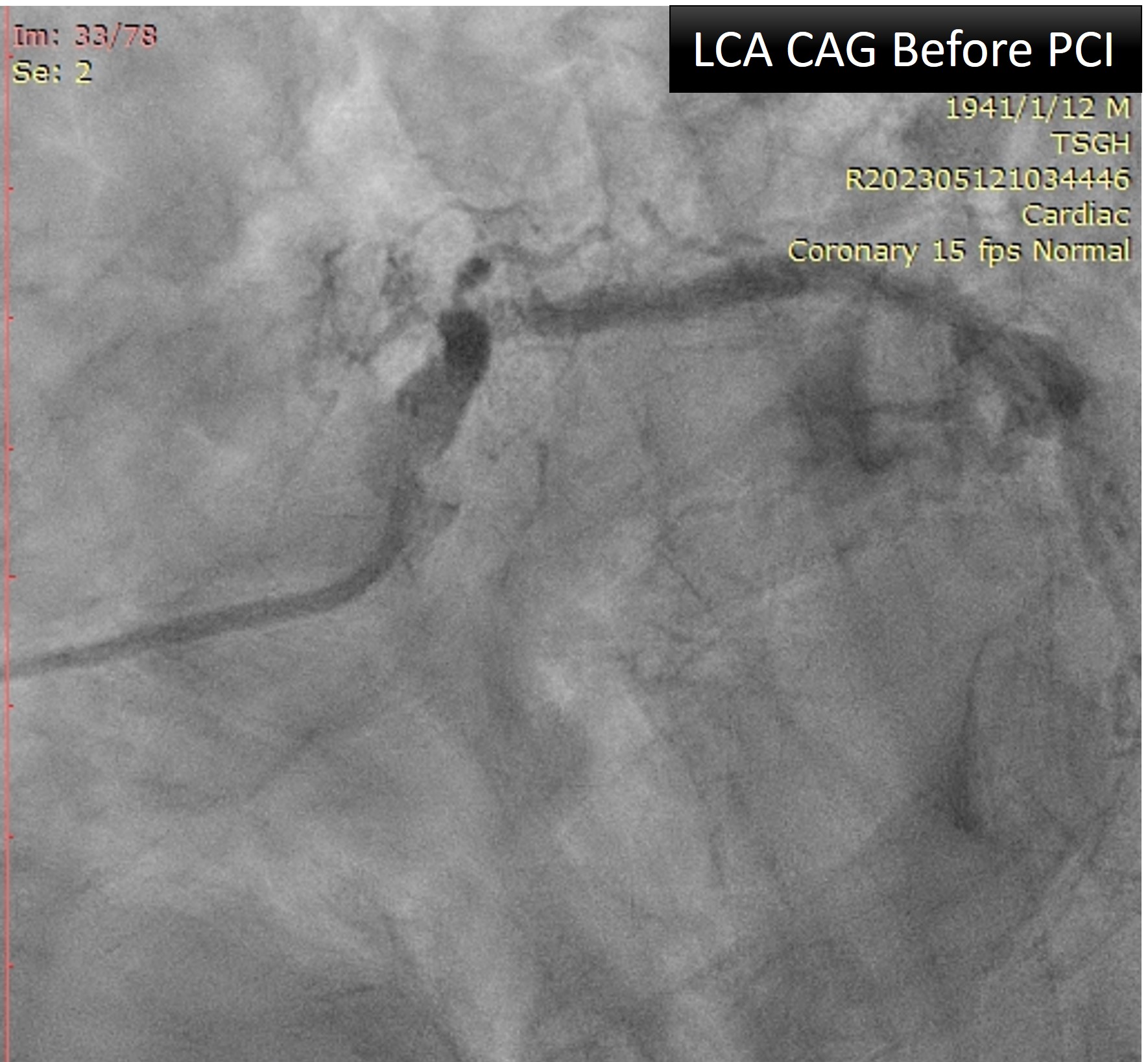
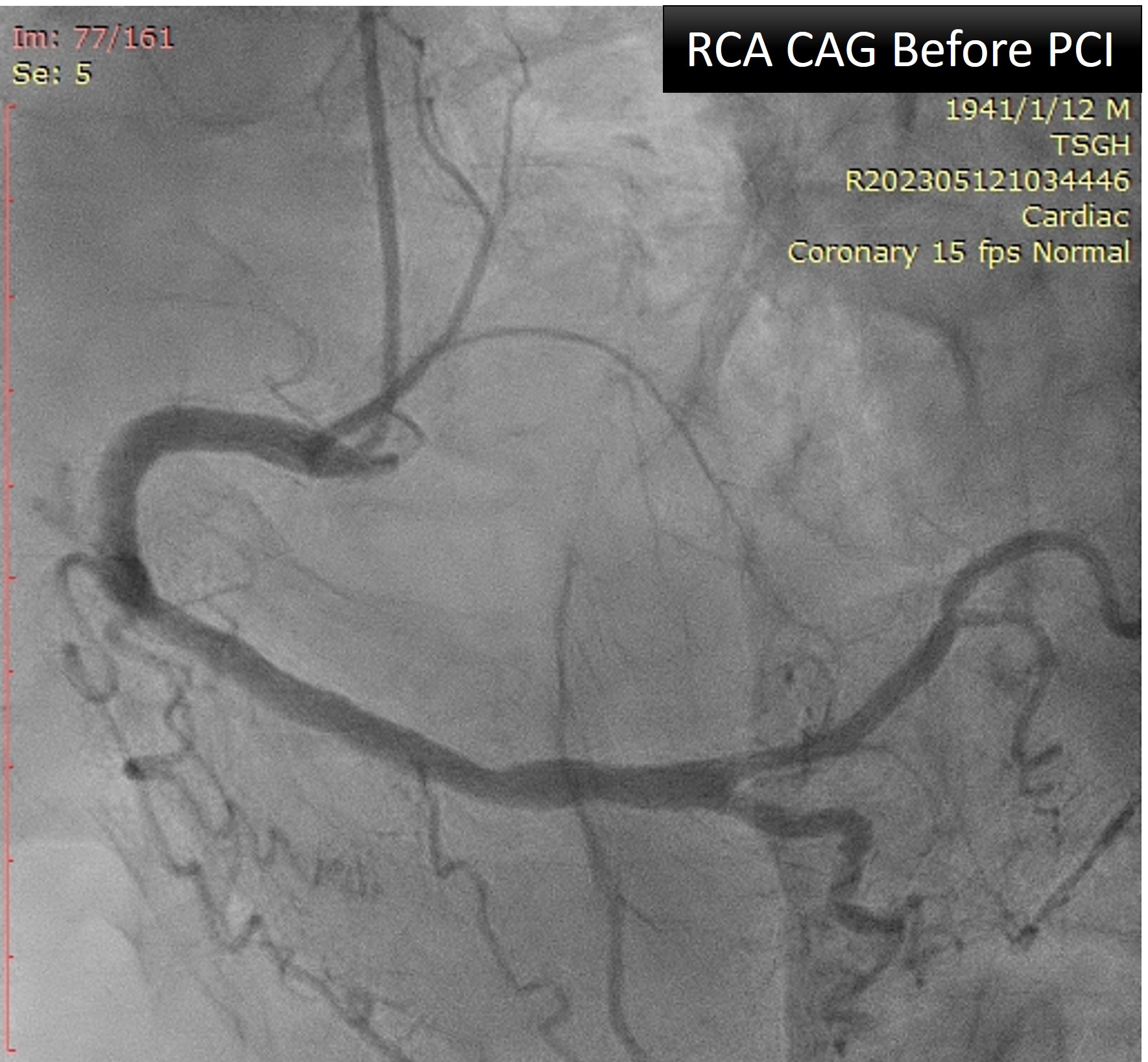
1. LMCA: Patent2. LAD: - Ostium: CTO3. LCx: - M/3: Tubular lesion, max 60% stenosis4. RCA: - PDA: Giving collateral to LAD via septal branches and LV apex
Interventional Management
Procedural Step
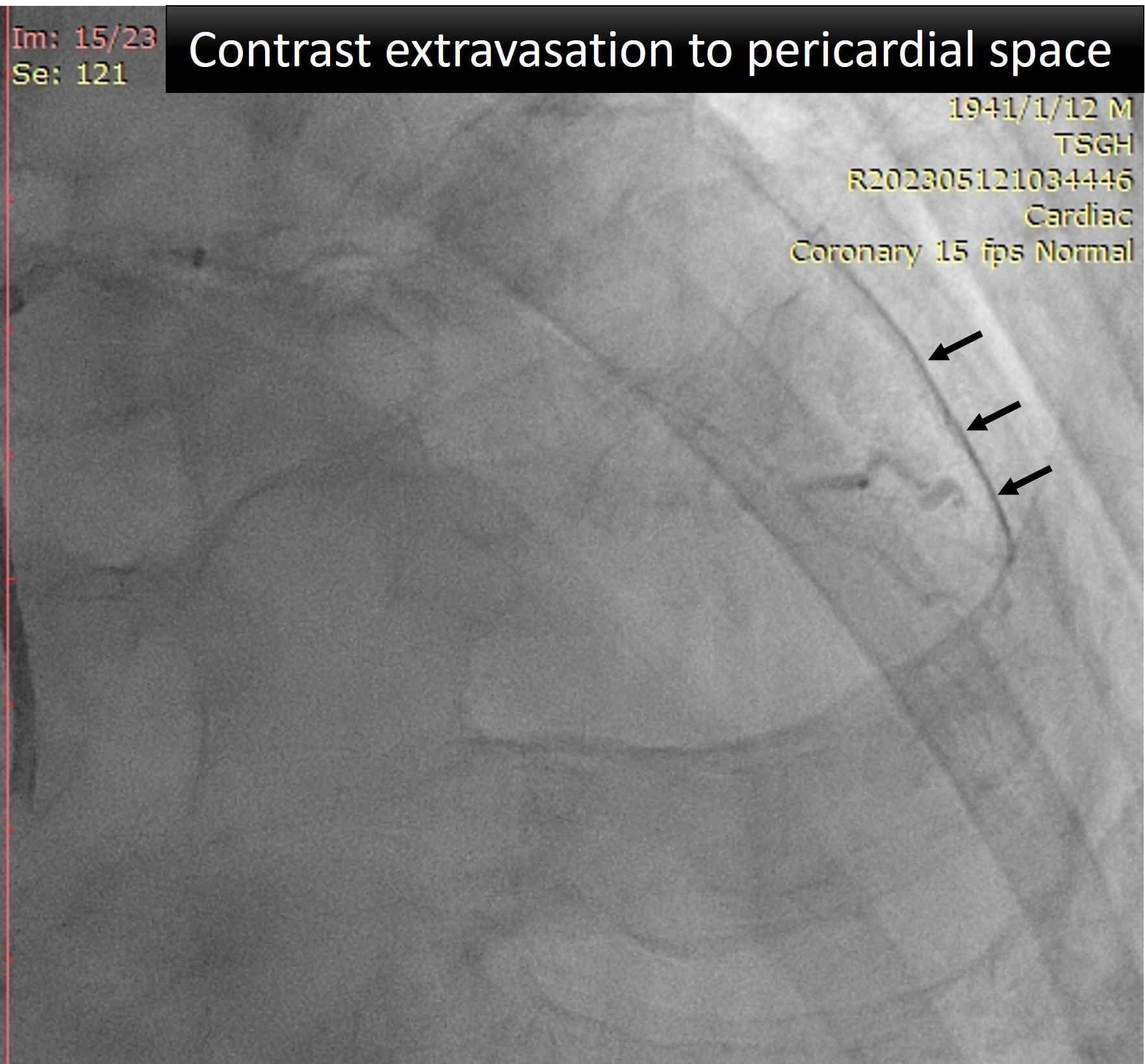
The coronary angiography showed CTO of LAD ostium and absence of significant RCA lesions with collaterals to the LAD via the septal branches and the LV apex. Two soft wires were inserted in LCx and ramus intermedius. After IVUS localization of LAD ostium, wiring of LAD with support of a Crusade Type R (Kaneka) microcatheter was attempted several times by antegrade wire escalation. The CTO cap was penetrated by a Conquest Pro wire (ASAHI intecc), but the wire could only be guided into the second diagonal branch (DB2) when encounter a severe angulation. The DB2 ostium was POBA by a 1.0 mm balloon. With support of the microcatheter, the wire gained access to the main branch and successfully passed through the CTO lesion. A heavily calcified lesion at middle LAD was identified by IVUS, which could not be opened by NC balloons. Therefore, rotational atherectomy using a 1.25 mm burr was performed. Following rotablation, the lesion in middle LAD showed complete expansion with a 2.5 mm NC balloon. Two 2.5 mm drug-eluting stents were deployed from proximal to distal LAD resulting in TIMI 3 flow. However, cardiac arrest happened 30 minutes after closing the procedure. Moderate amount of pericardial effusion with RV collapse was disclosed on echocardiography. After ACLS and emergent pericardiocentesis, ROSC was achieved. Reviewing the angiography records, there was distal perforation of DB2 with contrast leakage to pericardial space, which might be caused by wire penetration.

Case Summary
CTO revascularization was performed to this patient due to ischemic cardiomyopathy with viable myocardium demonstrated by Thallium-201 MPI. Life-threatening cardiac tamponade occurred after successful revascularization of LAD CTO lesion. After emergent management, the patient was discharged 1 month later. In this case, distal coronary artery perforation during wire manipulation in the side branch is possibly the major cause of cardiac tamponade. We learned the lesson from this case that careful wire manipulation and detailed image assessment should always be reminded, especially in complex CTO-PCI.