
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-211
A Challenging Case of TAVR With Coronary Protection in a Patient With Low Anomalous Origin of Circumflex Artery
By Debdatta Bhattacharyya, Saurabh Dhumale
Presenter
Debdatta Bhattacharyya
Authors
Debdatta Bhattacharyya1, Saurabh Dhumale2
Affiliation
RN Tagore Hospital, India1, Narayana Health Rabindranath Tagore International Institute of Cardiac Sciences, India2,
View Study Report
TCTAP C-211
Structural - Aortic Valve Intervention - Coronary Artery Protection / Access
A Challenging Case of TAVR With Coronary Protection in a Patient With Low Anomalous Origin of Circumflex Artery
Debdatta Bhattacharyya1, Saurabh Dhumale2
RN Tagore Hospital, India1, Narayana Health Rabindranath Tagore International Institute of Cardiac Sciences, India2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
85 year old hypertensive gentleman presented with the history of shortness of breath (NYHA III) and recurrent episodes of admission with heart failure. On admission his vitals were stable, with cardiovascular examination revealing a Grade 4/6 systolic murmur in the aortic area while respiratory system did not reveal any abnormal findings. Clinically the patient did not have any signs of heart failure. He was posted for TAVR after brief oral diuretic therapy.


Relevant Test Results Prior to Catheterization
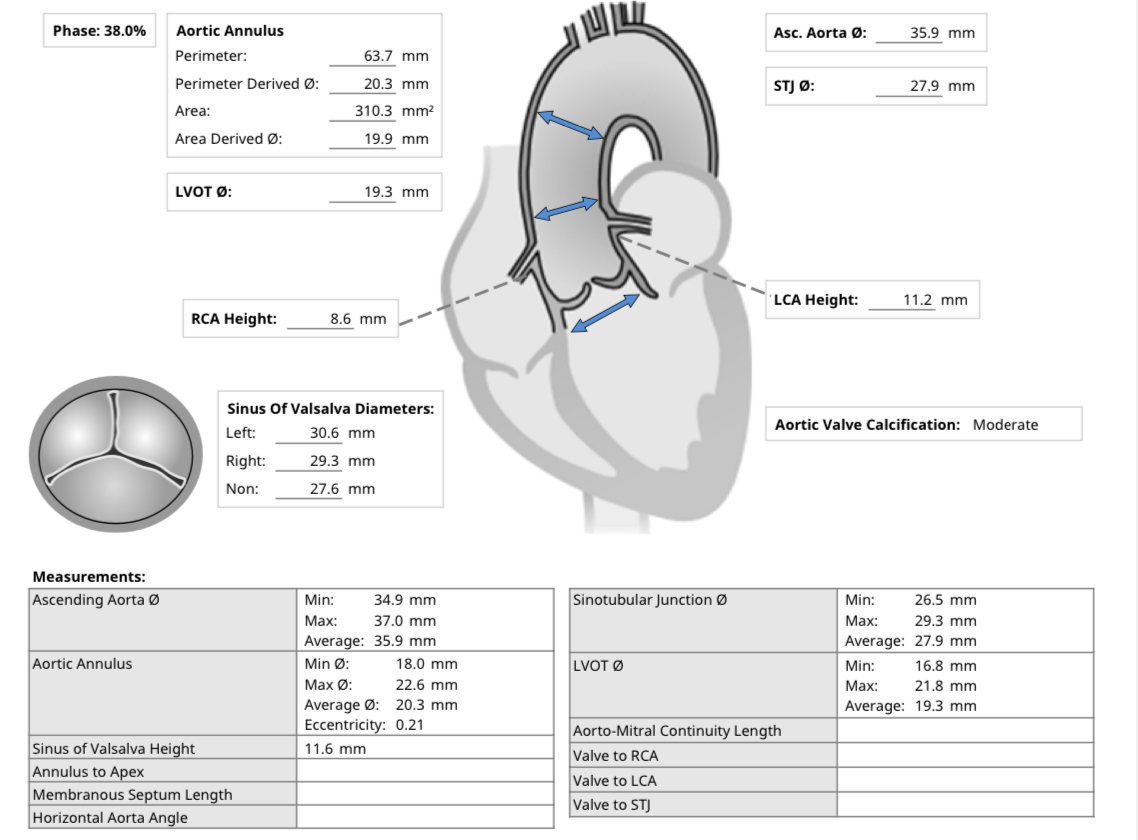
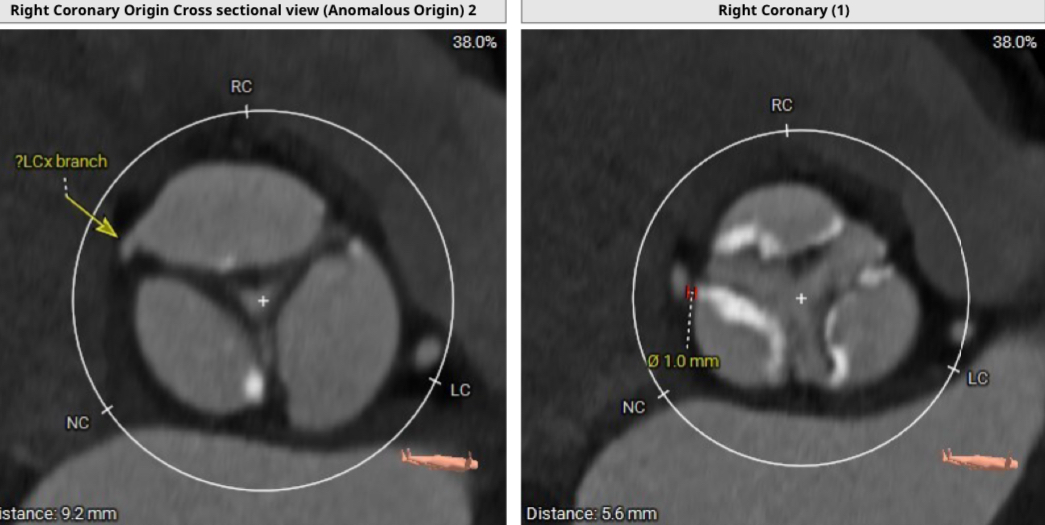
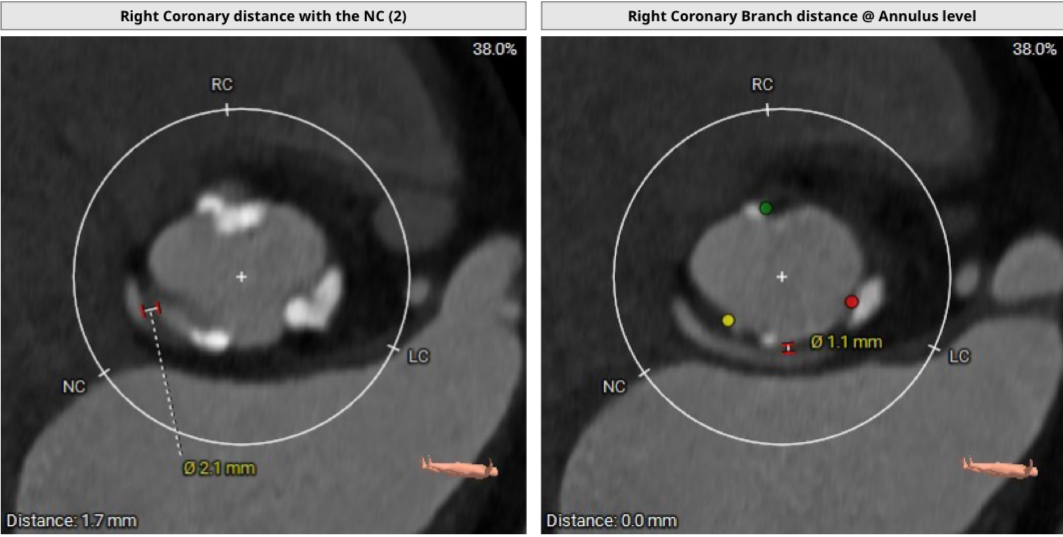
Patient's echocardiogram revealed severe calcific aortic stenosis (103mmHg Peak, 65mmHg mean gradients) with mild aortic regurgitation normal LV function and no mitral regurgitation or pulmonary hypertension. His CT analysis (TAVI Protocol) revealed a tricuspid aortic valve, moderate calcification extending into LVOT. What was peculiar in this case was that the LCX had an anomalous origin from the right cusp which was also lower down with a course between the aortic root and pulmonary artery.

Relevant Catheterization Findings
Coronary angiography confirmed the CT findings of a low and anomalous origin of circumflex with course traversing between aortic root and pulmonary artery. Due to the said origin and course, patient was at a high risk of circumflex occlusion both at the ostium and/or along its course around the aortic root. Anticipating this risk, it was decided to proceed with an upfront coronary protection strategy.

Interventional Management
Procedural Step
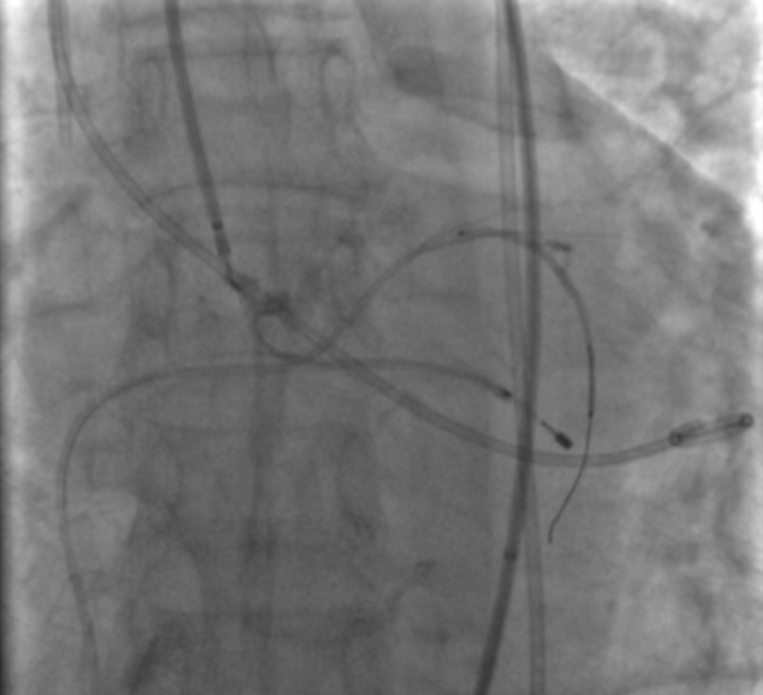
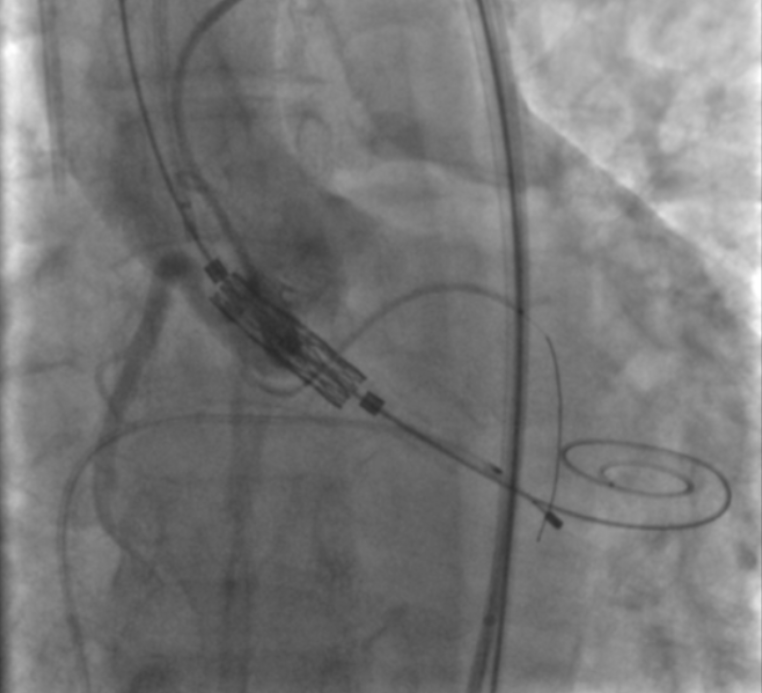
After a fluoro guided puncture from left CFA, anomalous LCX was engaged with MP 1 catheter. A 3X38mm DES was placed in distal anomalous LCX via a guideliner over a 0.014'' Sion Blue wire. After USG guided puncture of CFA, a 14F Python sheath was placed with the tip in the descending aorta. Valve was crossed with a straight tipped wire which was exchanged with a Safari Extra Small wire. Myval 21.5 was maneuvered over a Navigator delivery system, positioned under fluoroscopic guidance and deployed with rapid pacing at nominal pressure. However immediate aortogram post TAVI revealed no flow in the anomalous circumflex and the patient's hemodynamics deteriorated. Pre-positioned 3X24mm DES was pulled back in desired location and deployed so as to protect the ostium of the anomalous circumflex. After implantation of the proximal stent, a compression was noted in the mid-segment of the vessel, which was stented with a 3X38mm DES. There was no residual trans/para-valvular AR. Invasive gradient across aortic valve dropped from 110 mmHg to 0mmHg. Patient hemodynamics settled soon, and he was discharged in a stable condition after 2 days.


Case Summary
Low coronary height is an adverse feature for TAVI as there is a risk of coronary occlusion . This takes place due to lateral and upward displacement of the aortic leaflets on valve deployment. Usually this is tackled by the technique of chimney stenting. In our patient the challenge of coronary protection was compounded by the anomalous origin and course of the circumflex artery. This neccesitated protection both at the ostium as well as in the mid-segment where the artery was compressed due to its anomalous course between the aorta and the pulmonary artery as it became apparent after valve deployment. Our case was a demonstration that this can be done successfully in a difficult anatomy.