
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-212
Valve-In-Valve TAVR in a Patient of Degenerated Trifecta-21 With Severe Aortic Regurgitation and History of Implantation of AAA Stent Graft for Abdominal Aortic Aneurysm
By Debdatta Bhattacharyya, Manik Chopra, Snehil Goswami
Presenter
Snehil Goswami
Authors
Debdatta Bhattacharyya1, Manik Chopra2, Snehil Goswami3
Affiliation
RN Tagore Hospital, India1, NH-Rabindranath Tagore International Institute of Cardiac Sciences, India2, NH MMI Hospital, India3,
View Study Report
TCTAP C-212
Structural - Aortic Valve Intervention - Valve in Valve TAVR
Valve-In-Valve TAVR in a Patient of Degenerated Trifecta-21 With Severe Aortic Regurgitation and History of Implantation of AAA Stent Graft for Abdominal Aortic Aneurysm
Debdatta Bhattacharyya1, Manik Chopra2, Snehil Goswami3
RN Tagore Hospital, India1, NH-Rabindranath Tagore International Institute of Cardiac Sciences, India2, NH MMI Hospital, India3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 77 year old gentleman presented with severe shortness of breath (NYHA III) with recent history of recurrent hospital admissions (3 episodes) with heart failure. On examination, he was average built, conscious co-operative with bounding regular pulse and a wide pulse pressure (BP: 126/40mmHg). His cardiovascular examination revealed a high pitched decrescendo diastolic murmur. Chest examination did not have any significant findings.
Relevant Test Results Prior to Catheterization
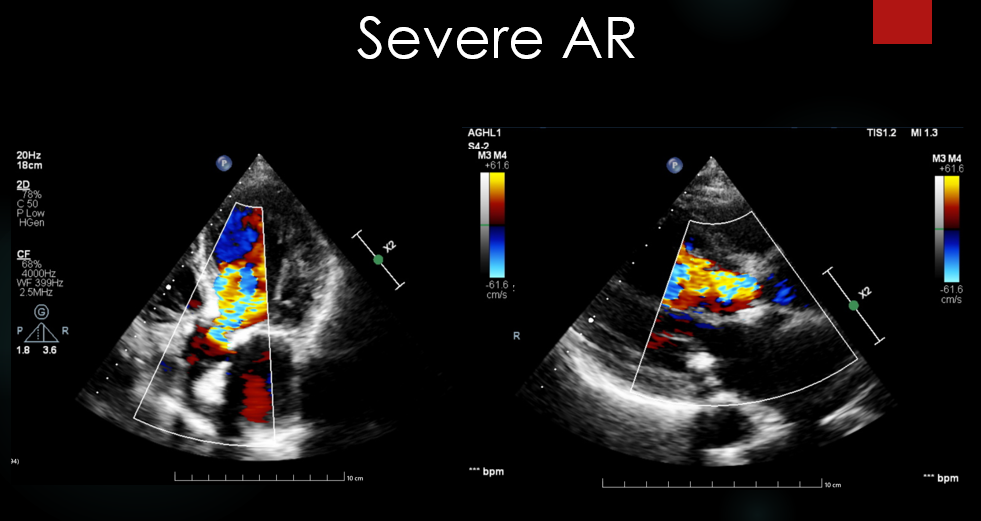
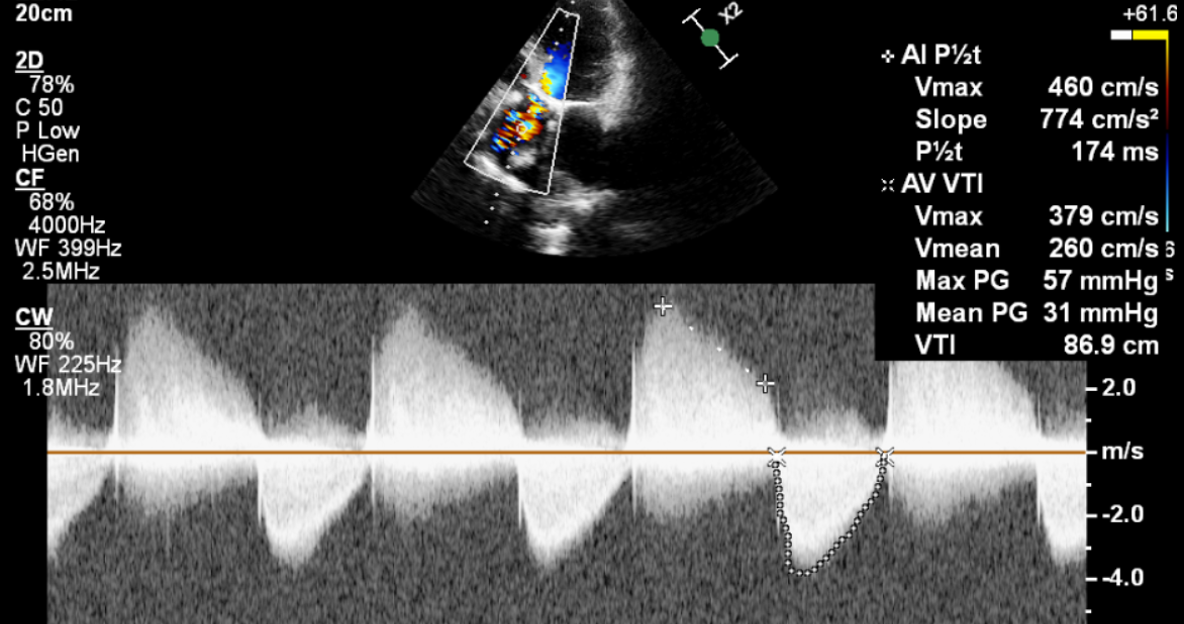
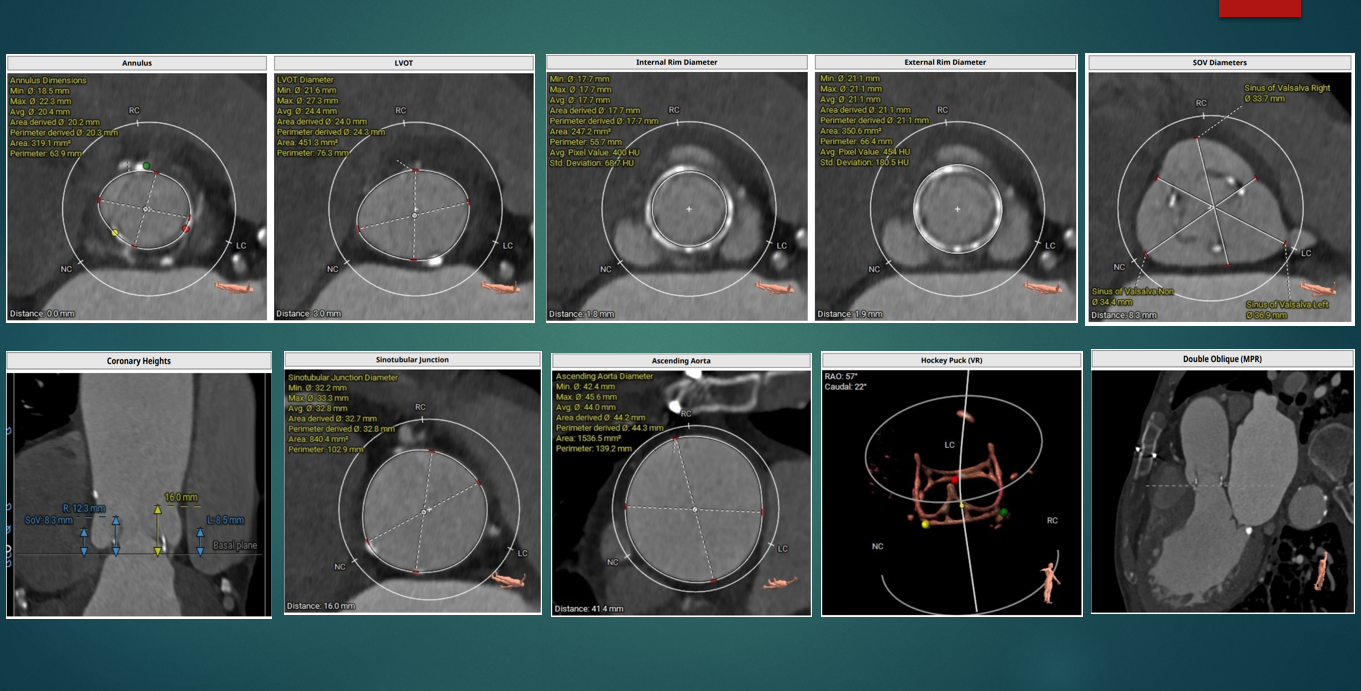
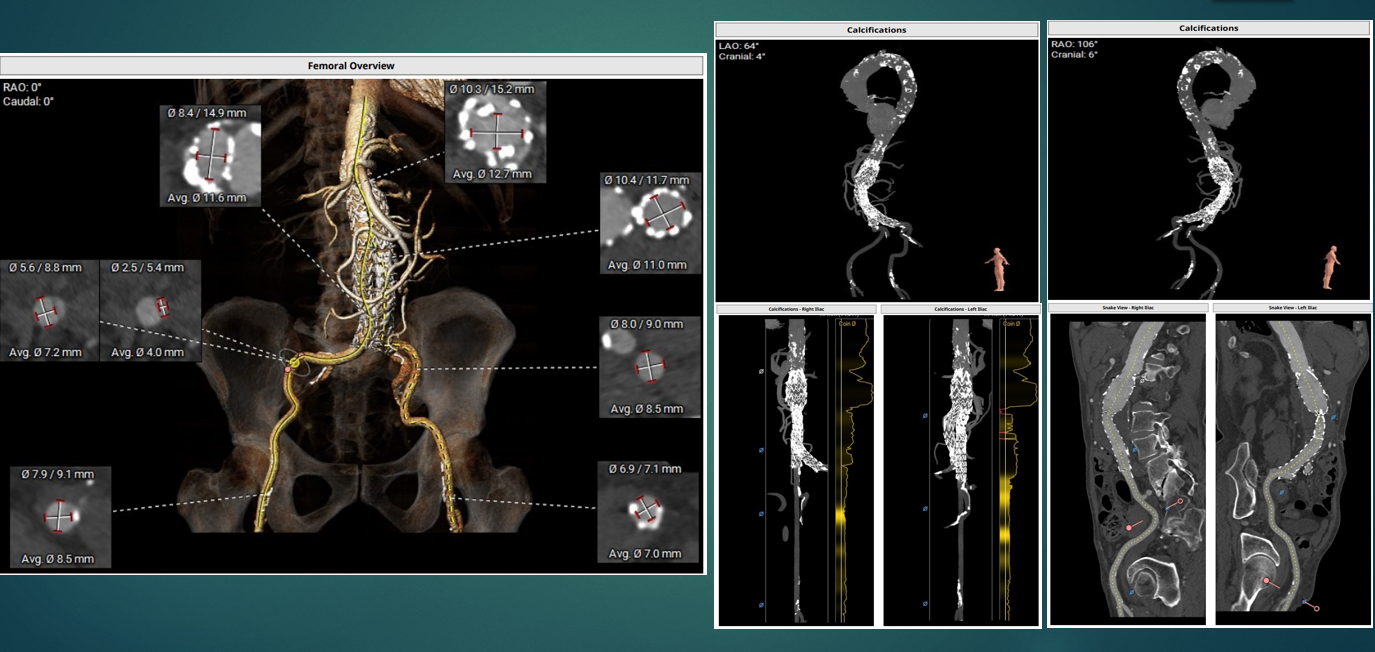
His 12 lead ECG showed sinus rhythm without any conduction abnormalities. ECHO revealed a bioprosthetic valve at aortic position with degenerative changes of the leaflets and severe transvalvular aortic regurgitation. CT analysis (TAVI Protocol) revealed aortic annulus 20.3mm in diameter, the annulus to LCA Height was 10.6mm, RCA height was 7.1mm. Iliofemoral analysis showed adequate sized peripheral arteries with tortuous femoral and external iliac arteries and a AAA graft .The SOV were large .

Relevant Catheterization Findings
Aortogram showed the Trifecta valve frame and severe AR . The aortic pressure confirmed the presence of AR .
Interventional Management
Procedural Step
Fluoroscopy guided femoral artery puncture was carried out . The aortic valve was crossed and the wire exchanged over a pigtail catheter to a SAFARI extra small wire. Pre-deployment aortogram revealed severe aortic regurgitation with aortic pressure of 110/16mmg (invasive). a 21.5 mm MYVAL was deployed at the implanters view in the lao caudal projection .Post deployment, there was no aortic regurgitation with significant improvement in the aortic diastolic pressure (110/60 mmHg).There was no evidence of coronary occlusion. Although the coronary heights were low we were confident that due to the large Sinus of Valsalva dimensions and the VIRTUAL VALVE TO CORONARY DISTANCE , the risk of occlusion was minimal.

Case Summary
Current surgical bioprosthetic valves in the aortic position tend to degenerate after 8-10 years resulting in severe AS or like in this case severe AR. Both balloon expandable and self expanding valves have been used to treat ViV lesions. The Trifecta valve cannot be cracked with balloon dilatation; since the patient had pre-dominant AR and there was no evidence of patient prosthesis mismatch with the first valve with a 21mm TRIFECTA we concluded it would be safe to implant a 21.5 mm MYVAL as a valve in valve in this patient . Our conviction was borne out by the satisfactory gradient post procedure which remained stable at 22/13 mm hg at 3 months follow up.