
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-099
Stent Blooming Complication: Guide Extension Catheter Nightmare in Percutaneous Coronary Intervention
By Robin Hendra Wibowo
Presenter
Robin Hendra Wibowo
Authors
Robin Hendra Wibowo1
Affiliation
Pasundan University, Indonesia1,
View Study Report
TCTAP C-099
Coronary - Complex PCI - Long Lesion
Stent Blooming Complication: Guide Extension Catheter Nightmare in Percutaneous Coronary Intervention
Robin Hendra Wibowo1
Pasundan University, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
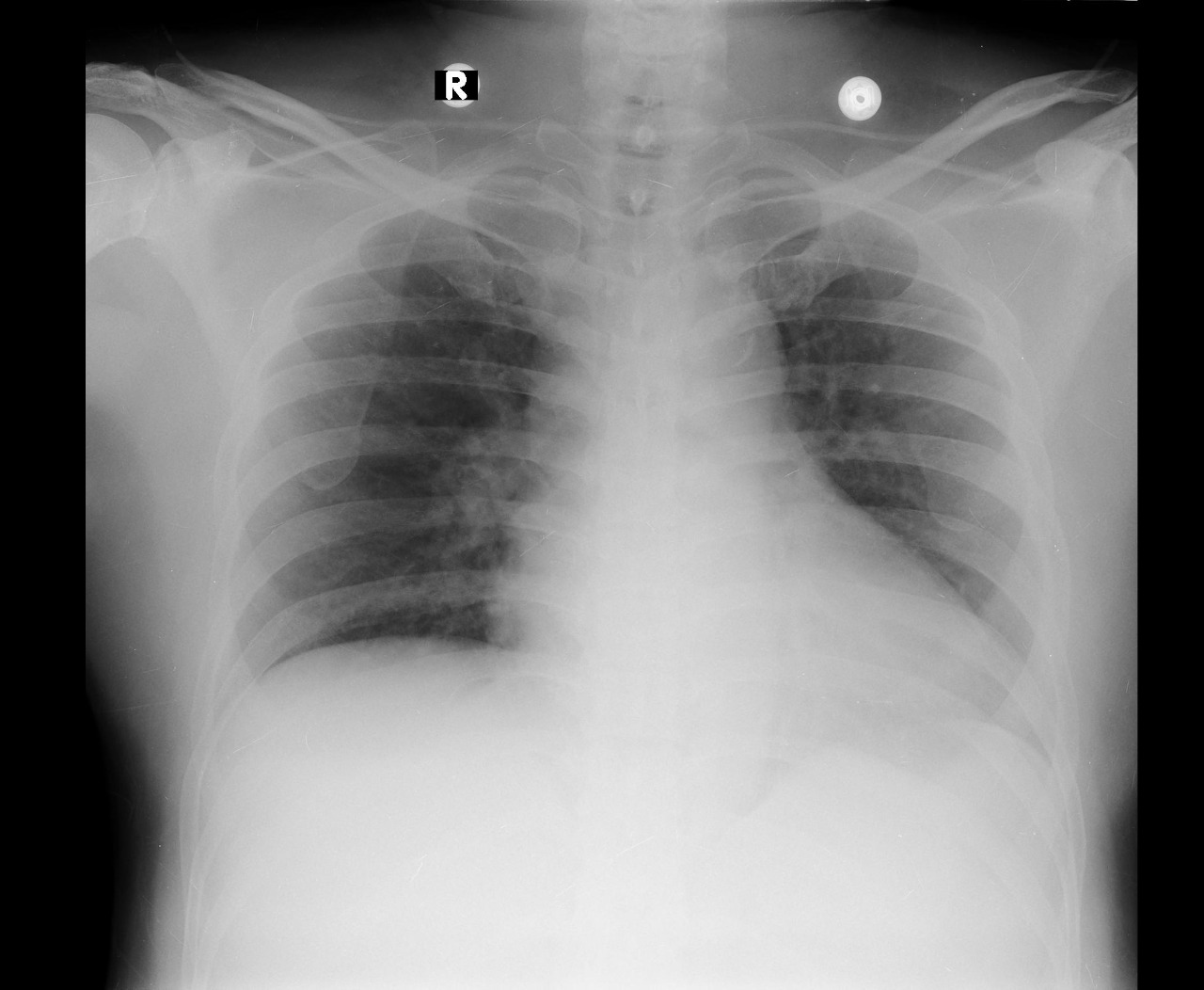
A 54-year-old male with history of active smoker presented to the emergency department complaining of chest pain with nausea, diaphoresis, and dyspnea. Vital signs at admission and physical examination were unremarkable.
Relevant Test Results Prior to Catheterization
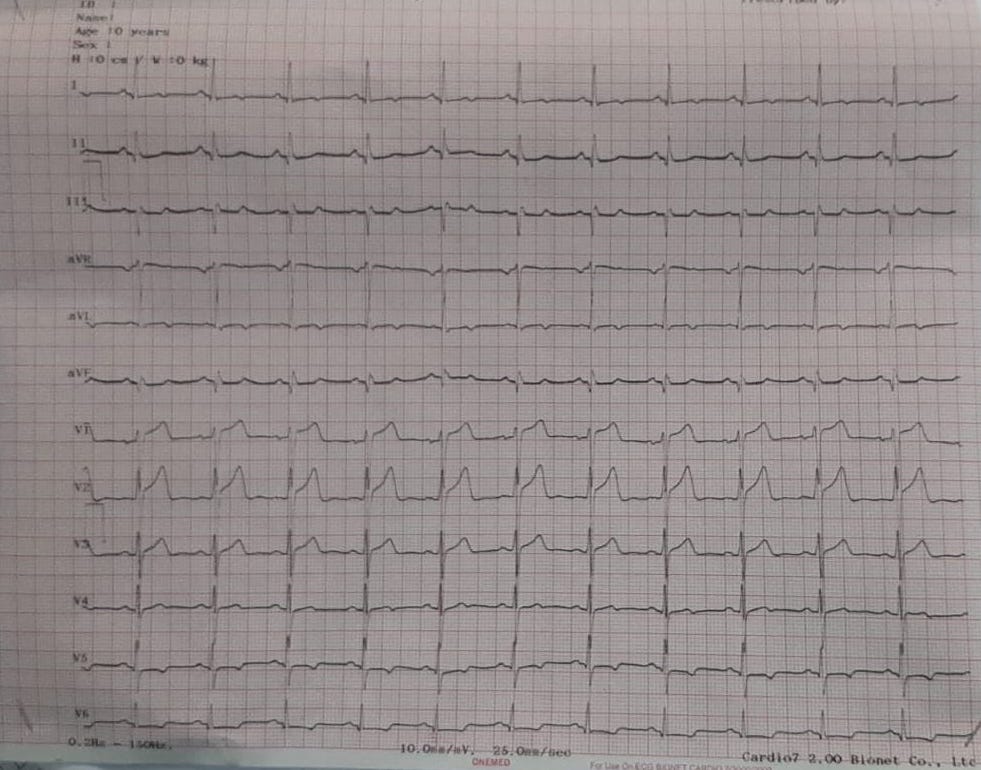
His Electrocardiogram (ECG) showed sinus rhythm, ST segment depression in anterolateral segments with elevated troponin I level (437ng/L). The diagnosis of NSTEMI inferior was established and referred to the cathlab for urgent PCI.
Relevant Catheterization Findings
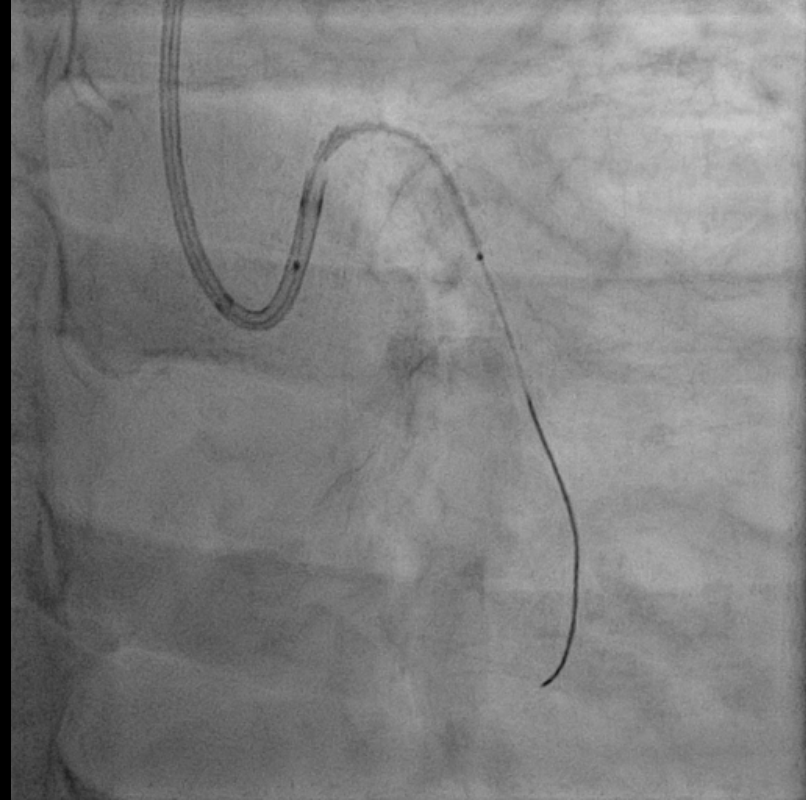
Angiography revealed three vessel disease. Left anterior descending artery (LAD) showed dual anatomy. LAD1 showed diffuse severe stenosis of proximal-mid part and LAD2 showed diffuse mild stenosis. Left circumflex (LCx) artery showed moderate ostial stenosis and severe diffuse stenosis proximal-distal part. The right coronary artery (RCA) showed chronic total occlusion of the proximal part and the distal portion receives collateral from the AM branch and distal part of LAD (Rentrop II).
Interventional Management
Procedural Step
PCI was conducted using guide catheter EBU3.5/6F, A 0.014-inch floppy guidewire and was placed in distal LCx. Predilatation was done using semicompliant 2,0 x 15mm and 2,5x15 mm balloon at up to 15 atm. There was difficulties in delivering the stent because of tortuosity and lack of support from the guiding catheter, we decided to add support with 6F guide extension catheter. We encountered distal stent blooming because of longitudinal stent deformation while delivering the stent DES Yukon 2.75x40 mm. The bloomed stent was successfully extracted. After femoral access crossover, stenting was performed using guide extension catheter support with DES Promus Premier 2.5x38 mm in proximal-distal LCx at 14 atm. Contrast injection showed TIMI Flow III, without dissection nor residual stenosis. Patient was dismissed from hospitalization without further complication.


Case Summary
We reported a 54-year-old male with NSTEMI and urgent PCI with guide extension catheter complication of undeployed stent damage. The bloomed stent was successfully extracted manually without further complications.