
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-118
Stuck Wire in a Calcific Coronary Artery
By Richa Sharma
Presenter
Richa Sharma
Authors
Richa Sharma1
Affiliation
Shri Mahant Indiresh Hospital, Dehradun, India1,
View Study Report
TCTAP C-118
Coronary - Complication Management
Stuck Wire in a Calcific Coronary Artery
Richa Sharma1
Shri Mahant Indiresh Hospital, Dehradun, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
73 year old male , K/C/O CAD/ P/AICD (9monthsback) p/w c/o recent onset rest angina 4 days back in our emergency.

Relevant Test Results Prior to Catheterization
• Echowas s/o LVEF -30%, mildly dilated LA/LV, mild MR, anterior, anterolateral andinferior wall hypokinetic.
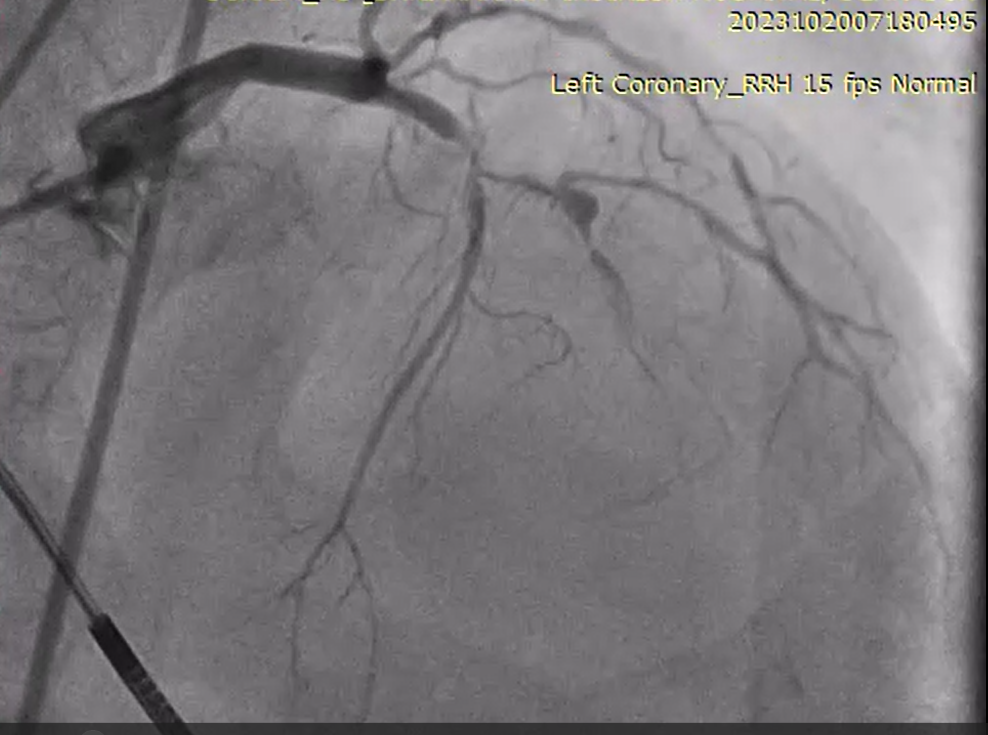
Relevant Catheterization Findings
• CAG-RCA 99% terminating into 100% CTO


Interventional Management
Procedural Step
• FielderFCwith MC support in RCA but wire cudn’t cross the tortous lesion 1.5*15 mm balloon taken and inflated at thesite of stuck wire


Wire got space and came out
Case Summary
The entrapment, fracture anddislodgement of diagnostic or therapeutic devices within the coronarycirculation during a procedure are a rare complication occurring in 0.2–0.8% ofcases.