
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-024
Mechanical Thrombosuction to Rescue for On-Table Myocardial Infarction Due to Clot Migration
By Prabesh Neupane, Anish Hirachan, Abdul Raqib Abd Ghani, Kamaraj Selvaraj
Presenter
Prabesh Neupane
Authors
Prabesh Neupane1, Anish Hirachan2, Abdul Raqib Abd Ghani3, Kamaraj Selvaraj4
Affiliation
Shahid Dharmabhakta National Transplant Centre, Nepal1, Nepal Mediciti Hospital, Nepal2, Hospital Serdang, Malaysia3, Sultan Idris Shah Serdang Hospital, Malaysia4,
View Study Report
TCTAP C-024
Coronary - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Mechanical Thrombosuction to Rescue for On-Table Myocardial Infarction Due to Clot Migration
Prabesh Neupane1, Anish Hirachan2, Abdul Raqib Abd Ghani3, Kamaraj Selvaraj4
Shahid Dharmabhakta National Transplant Centre, Nepal1, Nepal Mediciti Hospital, Nepal2, Hospital Serdang, Malaysia3, Sultan Idris Shah Serdang Hospital, Malaysia4,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A man aged 70 years with underlying diabetes and prior Coronary Angioplasty to left Circumflex Artery presented to us with sudden onset of left sided chest pain for 2 hours duration. His Blood pressure was 110/70mmhg and pulse was 80 beats per minute. Oxygen Saturation was 95% in room air. Patient was taking aspirin and statin therapy and had his Ticagrelor stopped 2 weeks prior to presentation.

Relevant Test Results Prior to Catheterization
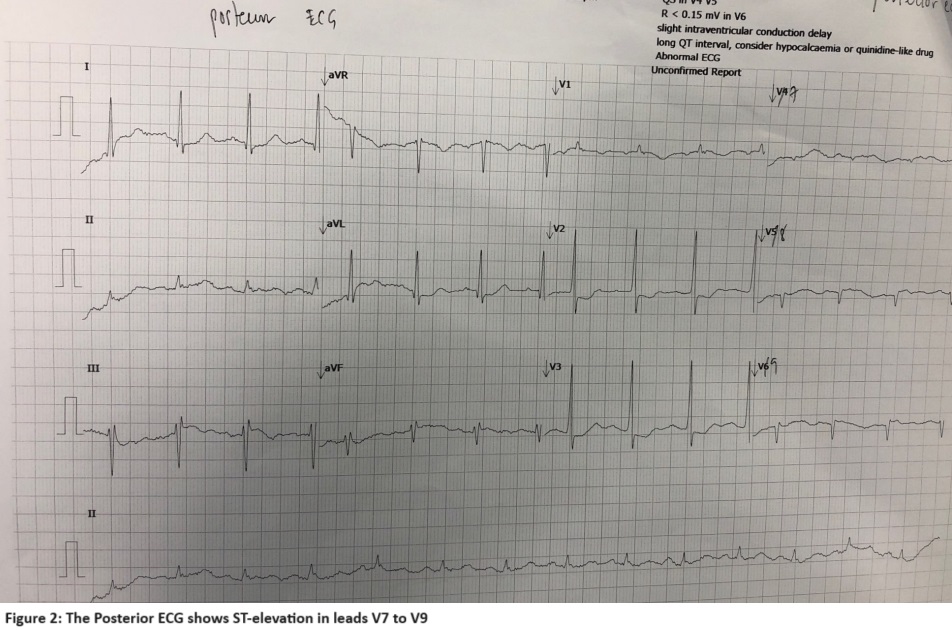
ECG revealed sinus rhythm with Heart rate of 79bpm, Significant horizontal ST depression was seen in Leads V1 to v4. (Figure 1)Another ECG with posterior leads showed ST elevation in leads V7 to V9.(Figure 2) A diagnosis of Acute Posterior wall MI was made. Patient received Ticagrelor 180mg and aspirin 300mg and was planned for Primary PCI. Chest X-Ray: Normal findings. Blood Investigations: Hemoglobin: 12.4 g/dL, Platelet: 215x10^9 g/L, Creatinine: 68 umol/L
Relevant Catheterization Findings
Diagnostic coronary angiography was done with a 5F Opti-torque catheter via right radial artery. Left coronary artery angiogram revealed co-dominant left system with complete thrombotic occlusion of proximal Circumflex artery at prior stented segment. LAD showed aneurysmal proximal to mid segment with minor disease. Right coronary angiogram revealed diffuse moderate disease in RCA. (Figure 3)The decision to proceed with Primary PCI of Left Circumflex was made.



Interventional Management
Procedural Step
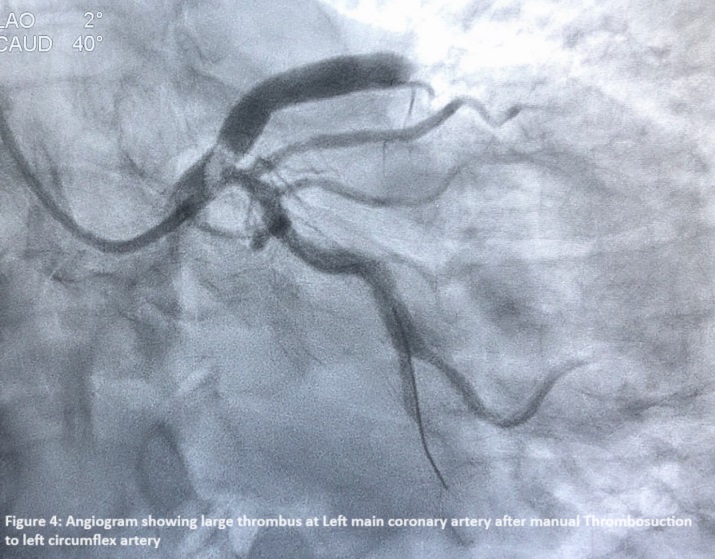
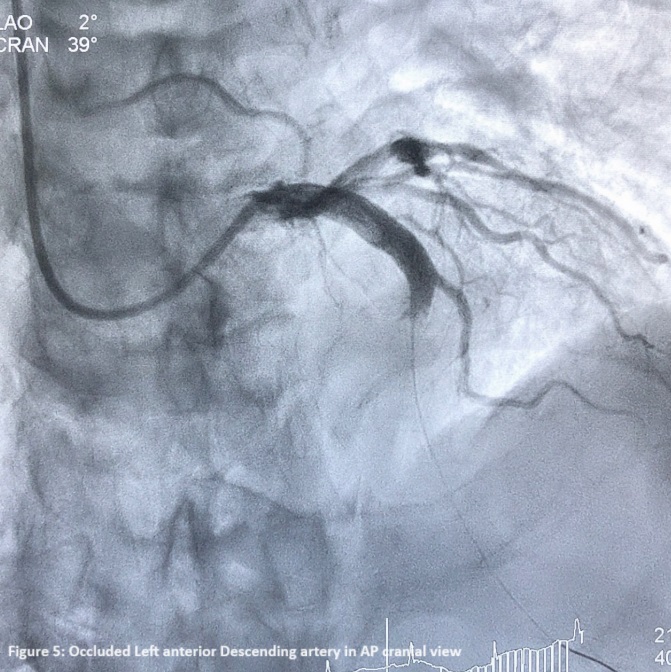
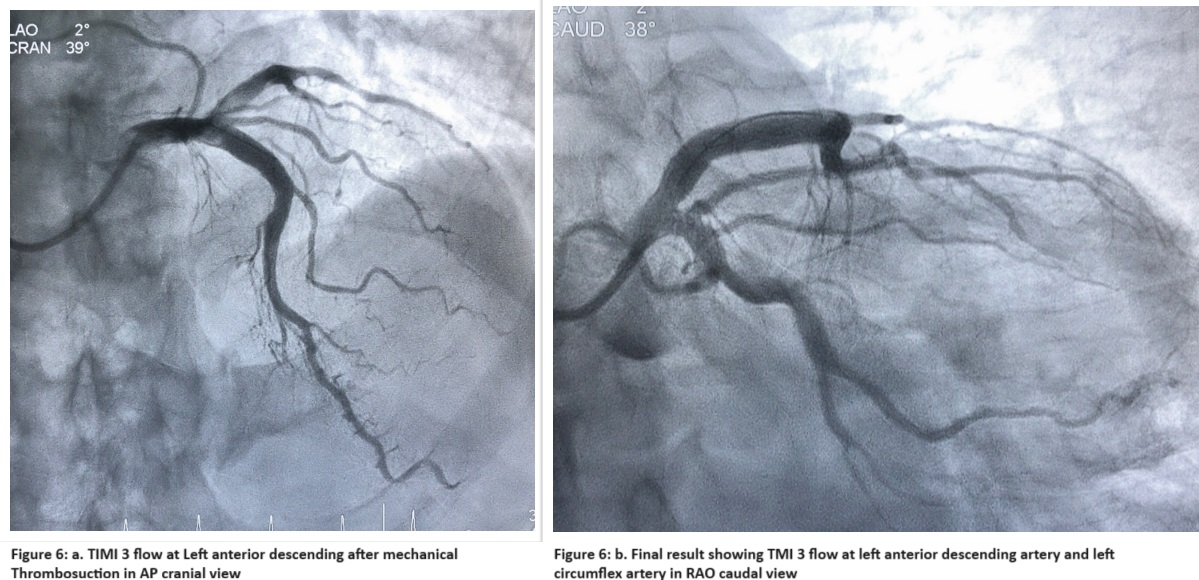
Patient received 100 IU/kg of unfractionated heparin. LCA was engaged with a 6 french EBU3.5 guiding catheter and lesion crossed with Sionblue Wire. Predilatation of the lesion with 3.0x15 mm NC balloon was done which revealed large thrombus burden. Patient received bolus of Tirofiban(25mcg/kg) and was started on maintenance dosage(0.15mcg/kg/min). Multiple Thrombosuction with manual syringe thrombosuction catheter were done after which TIMI III flow was appreciated in LCX. However a large mobile thrombus was seen at LMCA.(Fig.4) A floppy was quickly wired to LAD to notice complete occlusion of LAD by migrated thrombus. (Fig. 5). Patient was symptomatic with chest pain. ECG changes ensued and ionotrope was needed to maintain BP. In view of Large Thrombus, decision to use mechanical thrombosuction was made. 3 rounds of Thrombus aspiration was done with a 5 french mechanical coronary aspiration system (AngioJet Spiroflex VG , Boston Scientific). Following angiogram revealed TIMI 3 flow in LAD. Patient's hemodynamics improved and chest pain had abated. Balloon Dilatation with NC 4.0x15mm ballon @16atm was done at prior stented segment of LCX as per prior stent size. The final Angiogram showed TIMI 3 flow in both LAD and LCX. (Fig. 6) Patient was shifted to CCU with maintenance Tirofiban for 24 hours followed by LMWH. Relook angiography after 3 days showed good result. Patient was discharged on DAPT with Aspirin and Ticagrelor. Patient is doing well on planned followup.
Case Summary
In the setting of Primary PCI, Thrombosuction could still be a lifesaving modality. We presented a case where mechanical Thrombosuction device was safe and effective in rescue extraction of a huge thrombus. Multiple studies including TAPAS have demonstrated better reperfusion and clinical outcomes with thrombus aspiration. The risk of clot migration and possible stroke risk could possibly be avoided with upfront usage of advance mechanical Thrombosuction devices available now. Further studies with Novel Thrombosuction devices will likely evaluate the efficacy and safety of mechanical Thrombosuction in high thrombus burden cases.
|
Mohammad Shafiqur Rahman Patwary (NATIONAL INSTITUTE OF CARDIOVASCULAR DISEASES) Apr 25, 2024
|
|
| Good presentstion | |