
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-127
A Case of Stucked Rota Burr During Percutaneous Coronary Intervention
By Kee Wei Lee, Ng Kwang How, Ahmad Syadi Mahmood Zuhdi
Presenter
Kee Wei Lee
Authors
Kee Wei Lee1, Ng Kwang How1, Ahmad Syadi Mahmood Zuhdi2
Affiliation
University Malaya Medical Center, Malaysia1, University Malaya Medical Centre, Malaysia2,
View Study Report
TCTAP C-127
Coronary - Complication Management
A Case of Stucked Rota Burr During Percutaneous Coronary Intervention
Kee Wei Lee1, Ng Kwang How1, Ahmad Syadi Mahmood Zuhdi2
University Malaya Medical Center, Malaysia1, University Malaya Medical Centre, Malaysia2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
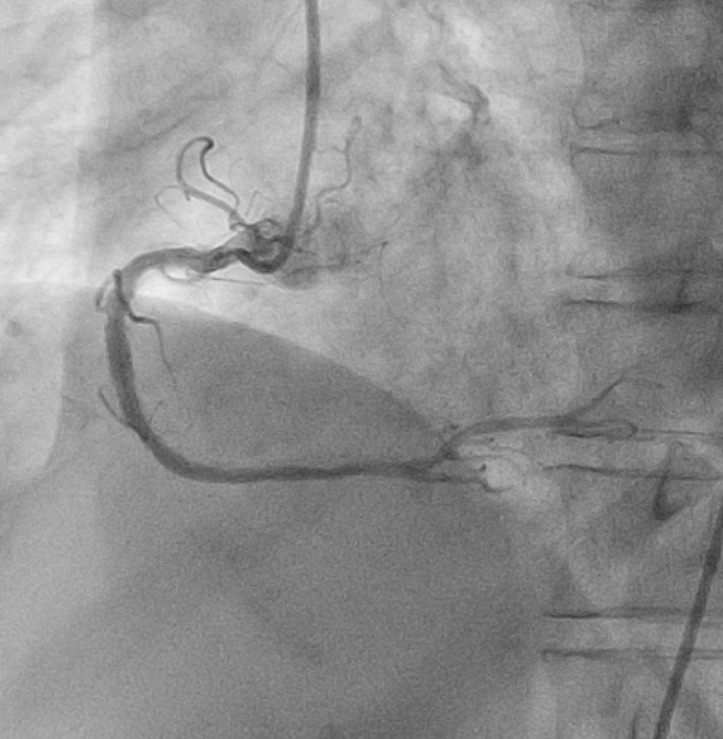
A 65-year old female with background history of diabetes mellitus and coronary artery disease with history of percutaneous coronary intervention (PCI) to RCA in 2022, was electively admitted for staged PCI to the LAD. Physical examination was unremarkable and vital signs were stable.

Relevant Test Results Prior to Catheterization
Blood tests were normal. Troponin I was not raised. Electrocardiogram (ECG) showed sinus rhythm with poor R wave progression and T inversion at precordial leads V2-V6 and lateral leads I, aVL. 2D-echocardiogram showed LV ejection fraction (EF) of 40% by Simpson’s method with moderate global hypokinesia and normal chambers sizes.
Relevant Catheterization Findings
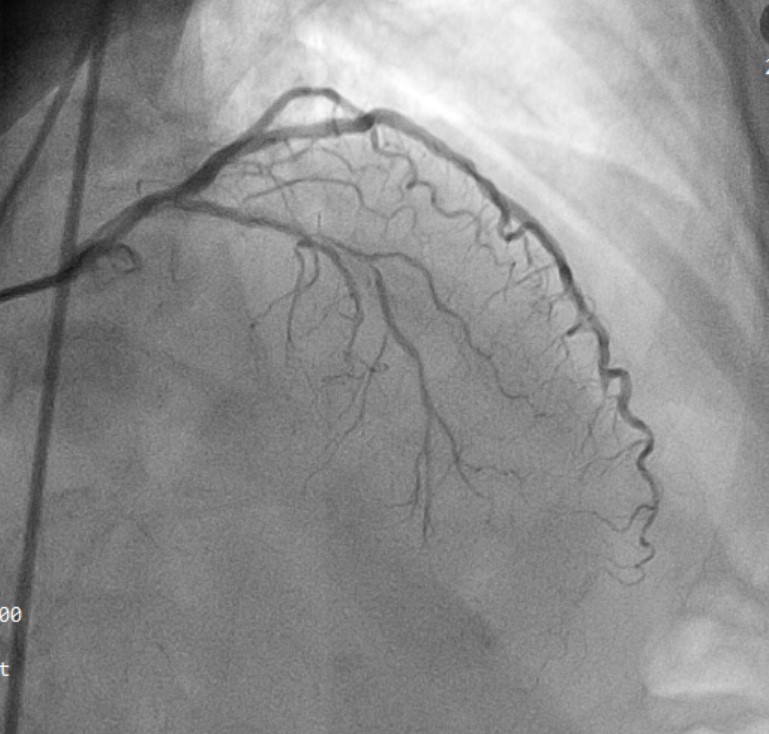
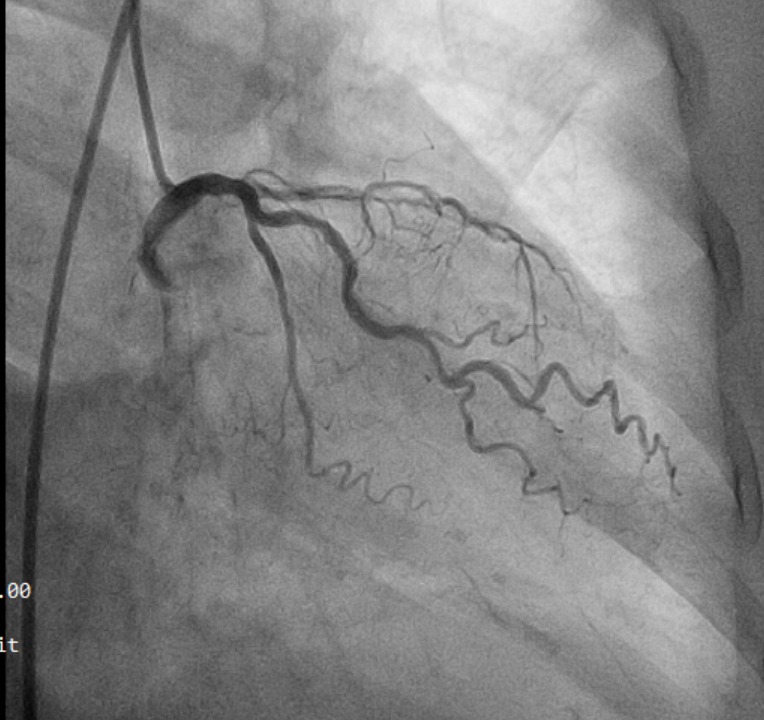
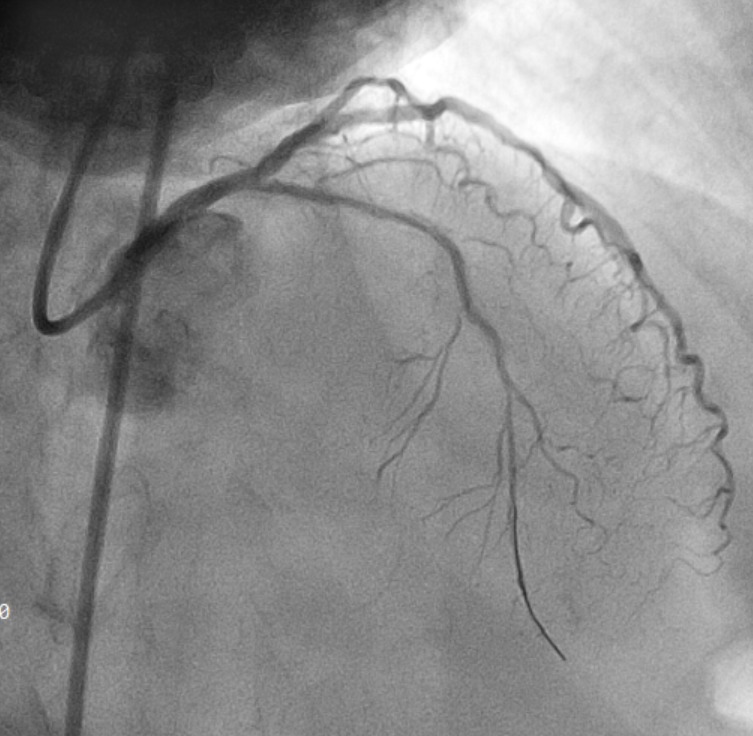
Coronary angiography showed smooth LMCA. There was calcified, severe stenosis at mid segment of LAD, mild plaque disease of LCx while the previous RCA stent was patent.
Interventional Management
Procedural Step
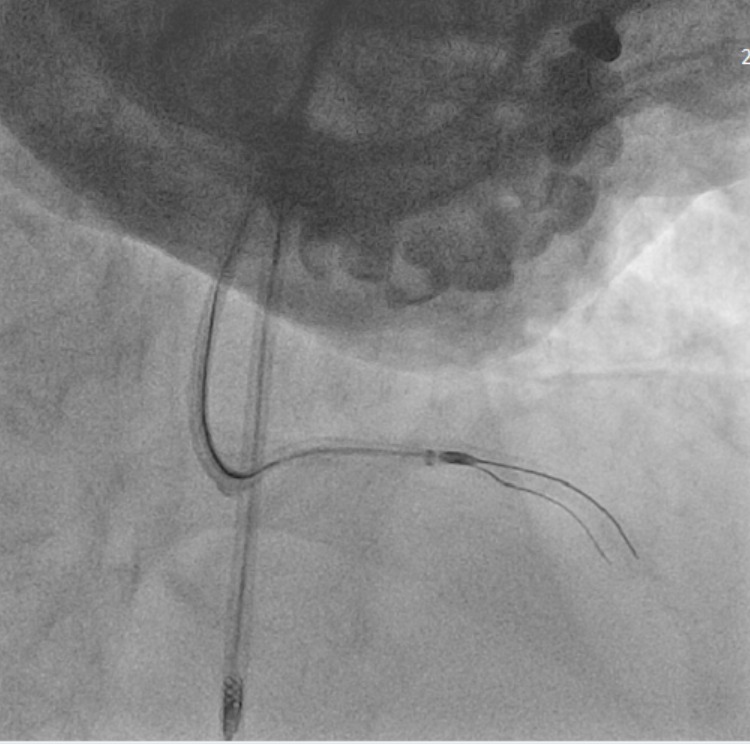
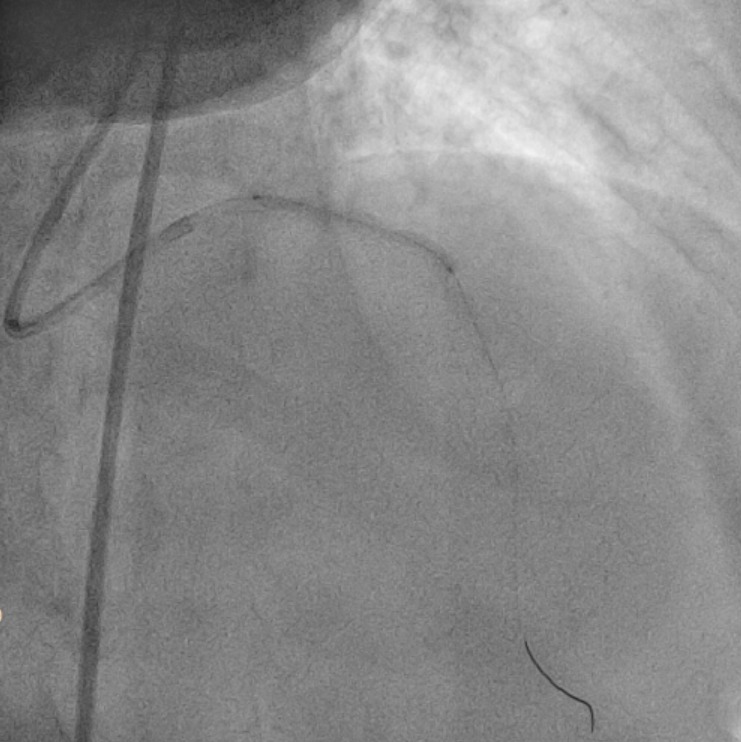
Vascular access obtained with transfemoral puncture with 7 Fr sheath. Guiding catheter XB 3.5 (Cordis, USA) 6Fr was used to engage the left coronary ostium. Runthrough (Terumo, Japan) coronary wire was inserted with FineCross (Terumo, Japan) microcatheter support through distal LAD. Up-front IVUS was planned but unable to pass through the tight stenosis. Workhorse wire was changed to Rota Floppy (Boston Scientific,USA) and atherectomy was performed using RotaPro system (Boston Scientific,USA) with burr size 1.5 mm at 170 - 180 k rpm. Procedure complicated with stucked rota burr at LAD after 5 runs. Rota burr system was cut and its protective sheath removed. Trial to dislodge the burr using FineCross (Terumo,Japan) with Fielder XT wire (Asahi, Japan) and SC Sapphire (OrbusNeich, China) 0.85 x 5 mm and 1.0 x 5 mm balloons were unsuccessful. Next, trial with guide extension catheter Guidezilla (Boston Scientific, USA) using over-the-wire technique and traction applied. Rota burr and rota wire were retrieved successfully with no perforation. PCI to LAD was resumed. Noted there was type B dissection over mLAD with TIMI 3 flow. Lesion was further prepared with NC Sapphire (OrbusNeich, China) balloon 2.0 x 15 mm. OptiCross IVUS (Boston Scientific, USA) assessment of LAD noted 360 degree calcium at mLAD not ablated, other segments have demonstrable reverberation. Final decision was to treat with DCB Magic Touch (CMI, USA) 2.5 x 20 and 2.5 x 30 mm. Post PCI result was acceptable.
Case Summary
Entrapment of a rota burr or Kokeshi phenomenon is an infrequent complication that can occurred during PCI. Removal of the stuck burr can be achieved by surgical removal with subsequent coronary artery bypass surgery or percutaneous interventional techniques. There are a few ways that can be employed for retrieval of entrapped burr. In our case, we employed the technique of disassembly of the Rotablator system and using Guidezilla extension catheter to retrieve the stuck burr with controlled traction. Step-by-step retrieval approach with familiarities with techniques and devices are important to bail both the interventionist and patient from this complication.