
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-007
Successful Reperfusion With Intracoronary Thrombolysis via Aspiration Thrombectomy Catheter in ST-Segment Elevation Myocardial Infarction
By Polpat Euswas
Presenter
Polpat Euswas
Authors
Polpat Euswas1
Affiliation
Hua Hin Hospital, Thailand1,
View Study Report
TCTAP C-007
Coronary - ACS/AMI
Successful Reperfusion With Intracoronary Thrombolysis via Aspiration Thrombectomy Catheter in ST-Segment Elevation Myocardial Infarction
Polpat Euswas1
Hua Hin Hospital, Thailand1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
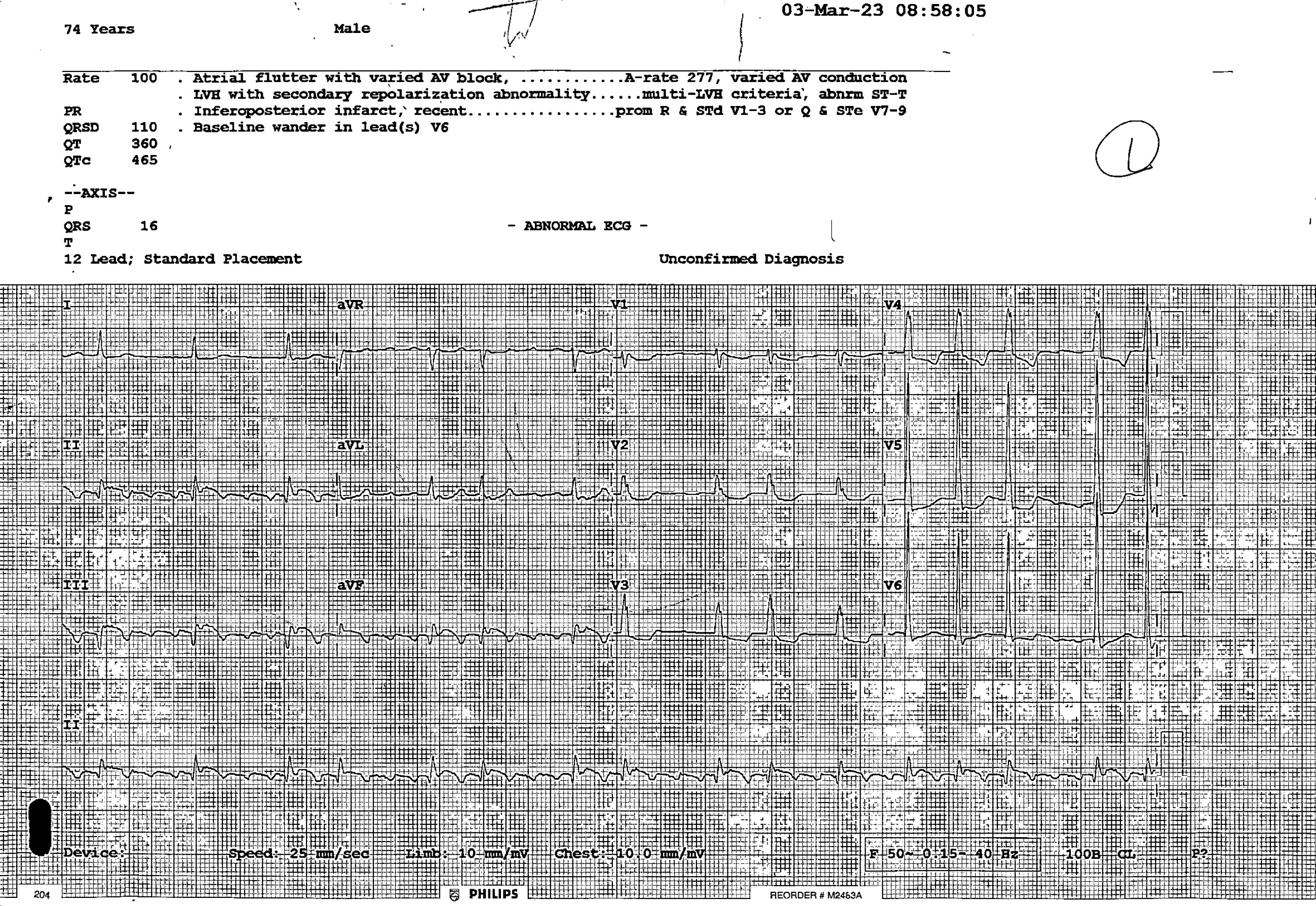
74 year-old male with hypertension, dyslipidemia and tobacco use, was presented with acute chest pain onset for 6 hours at the primary rural hospital. Blood pressure was 130 / 72 mmHg. Heart rate was 82 beat per minute. Respiratory rate was 20 per minute. Neither sign of heart failure nor neurological deficit were present.
Relevant Test Results Prior to Catheterization
ECG shown atrial flutter with ST elevation at lead II, III and AVF with ST depression at V2 to V5. The diagnosis was ST elevation myocardial infarction infero-posterior wall. The patient was referred to my PCI-center hospital for primary PCI strategy (referral time was 3 hours because of long distance).
Relevant Catheterization Findings
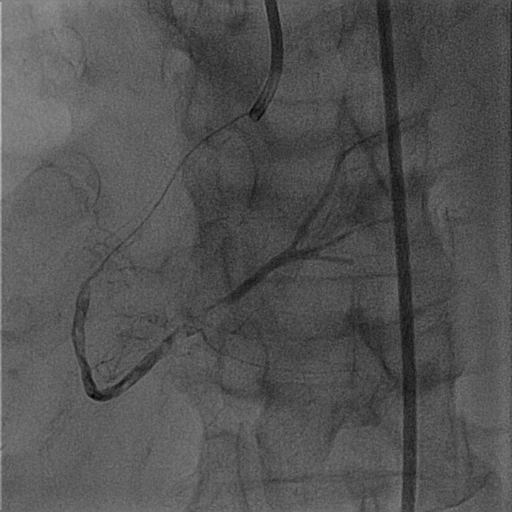
The primary PCI procedure was started with Judkin right guiding catheter for right coronary artery (RCA) angiogram and plan for PCI. The RCA finding was shown with 100 % thrombotic occlusion since ostial RCA, PCI procedure was immediately done without left coronary angiogram.

Interventional Management
Procedural Step
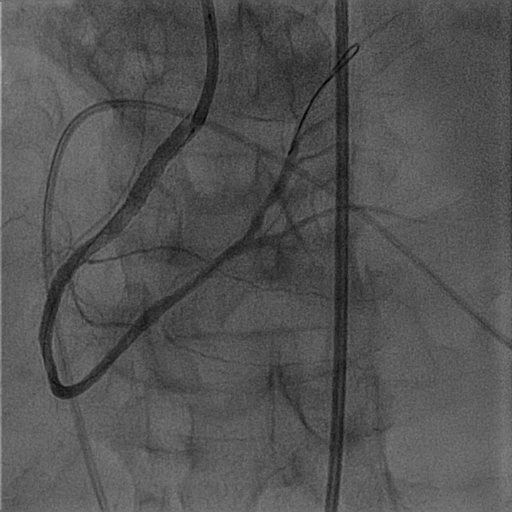
Guiding catheter was Judkin right (JR) 3.5 / 7 French. Guidewire with microcatheter was passed into RCA and confirmed with contrast injection via microcatheter. Massive thrombus along RCA was presence. The first strategy, aspiration thrombectomy was performed for 3 times, but the RCA flow was not good because of massive thrombus. The second strategy was low pressure balloon dilatation with semi-compliant balloon 2.5 / 15 mm. for 4 - 6 atm, but the result was poor. The next strategy was intracoronary thrombolysis (Alteplase), started with 5 mg via JR guiding catheter, after that no reflow and severe bradycardia were happening, thus internal temporary pacemaker was inserted. The next step was used intracoronary Alteplase administered via aspiration thrombectomy catheter with Guidezilla assist because the JR guiding was not had backup support. The Alteplase injection via aspiration thrombectomy catheter was successful (dose 5 mg, interval 5 minutes, total 2 doses). The cine was shown the thrombus was nearly disappeared with TIMI 3 flow. Then, semi-compliant balloon 2.5 / 15 mm was dilated at mid to ostial RCA. The drug eluting stents were placed with 3.0 / 38 mm and 3.5 / 23 mm from mid to ostial RCA, retrogradely overlapped. Final angiogram shown final TIMI 3 flow. Intra-aortic balloon pump was inserted for hemodynamic support.

Case Summary
STEMI with large thrombus burden was associated with poor prognosis, including procedural failure, abrupt vessel closure, recurrent myocardial infarction and death. There were many methods to reduce the thrombus load of patients with STEMI, such as distal protection device, thrombus aspiration, and glycoprotein IIb/IIIa antagonists, etc. This case was shown about the administration of low dose intracoronary thrombolysis strategy was significantly reduced residual thrombus after manual aspiration resulted in thrombus grade reduction, improved epicardial flow and tissue-level perfusion by dissolving thrombi at microvascular level. This strategy was safe without major bleeding complication.