
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-154
Impella Assisted Percutaneous Coronary Intervention for In-Stent Restenosis of Right Coronary Artery Stent Jutting Out Into Aorta for a Patient in Cardiogenic Shock
By Lakshmi Durga Kumaraguruparan, Subashini Subramanian, Nagendra Boopathy Senguttuvan, Ramesh Sankaran, Vinod Kumar Balakrishnan, S Sadhanandham, Thoddi Ramamurthy Muralidharan, Sadagopan Thanikachalam
Presenter
Lakshmi Durga Kumaraguruparan
Authors
Lakshmi Durga Kumaraguruparan1, Subashini Subramanian1, Nagendra Boopathy Senguttuvan1, Ramesh Sankaran1, Vinod Kumar Balakrishnan1, S Sadhanandham1, Thoddi Ramamurthy Muralidharan1, Sadagopan Thanikachalam1
Affiliation
Sri Ramachandra Institute of Higher Education and Research, India1,
View Study Report
TCTAP C-154
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
Impella Assisted Percutaneous Coronary Intervention for In-Stent Restenosis of Right Coronary Artery Stent Jutting Out Into Aorta for a Patient in Cardiogenic Shock
Lakshmi Durga Kumaraguruparan1, Subashini Subramanian1, Nagendra Boopathy Senguttuvan1, Ramesh Sankaran1, Vinod Kumar Balakrishnan1, S Sadhanandham1, Thoddi Ramamurthy Muralidharan1, Sadagopan Thanikachalam1
Sri Ramachandra Institute of Higher Education and Research, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
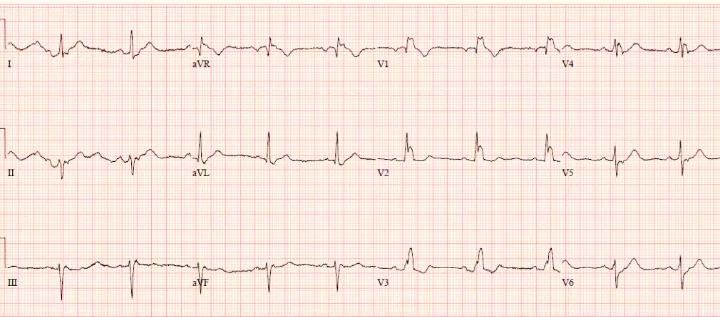
74 years old gentleman with prior CAD - AWMI in 2020 with PCI from LM to LAD, had AWMI in May 2022 with ISR of LM to LAD stent, for which PTCA was done. In November 2022, he had Unstable Angina with mild ISR of LM to LAD stent and Ostioproximal RCA long segment stenosis for which PCI was done. Presenting complaint was anginal chest pain for a week. Hypotension with cold peripheries was noted. CVS - normal heart sounds with no added sounds/murmurs. ECG showed RBBB,normal QTc and PR interval.
Relevant Test Results Prior to Catheterization
Transthoracic Echocardiogram done showed dilated LA, LV, LAD territory akinetic, RCA territory hypokinetic, basal lateral wall contracting well, severe LV systolic dysfunction with Grade III diastolic dysfunction and moderate MR.
Relevant Catheterization Findings
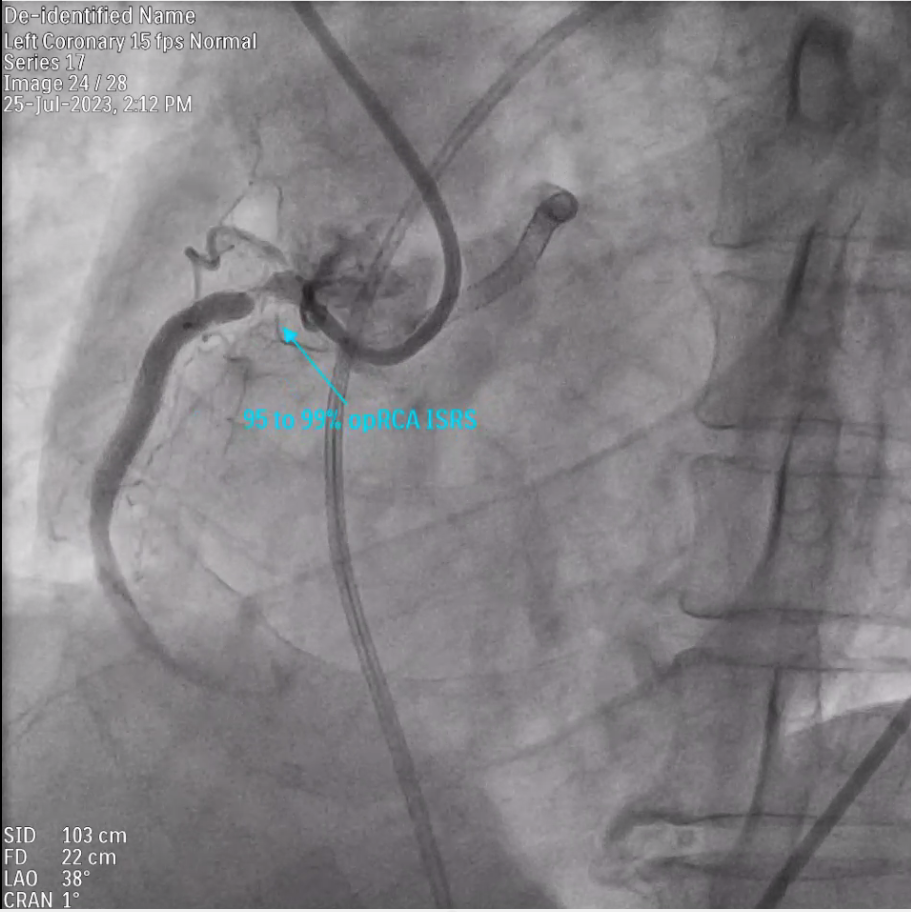
Coronary Angiogram done showed LMCA to mid LAD stent having mild ISR in its mid part and Proximal RCA Stent has 95% ISR.
Interventional Management
Procedural Step
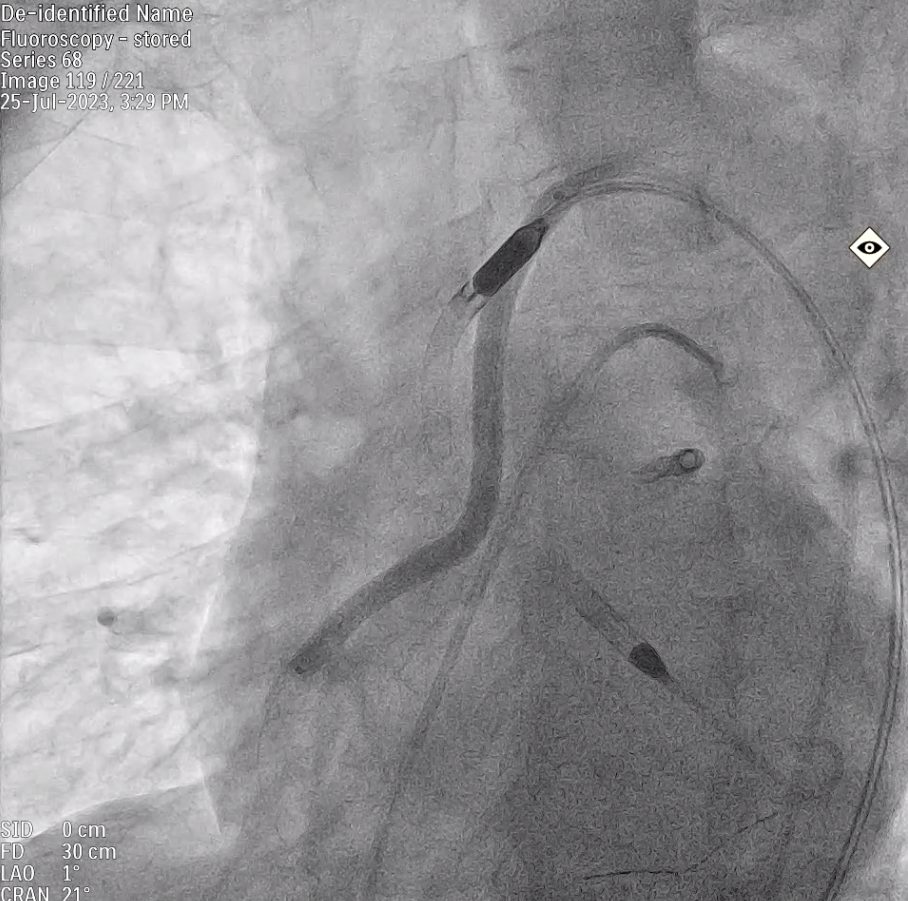
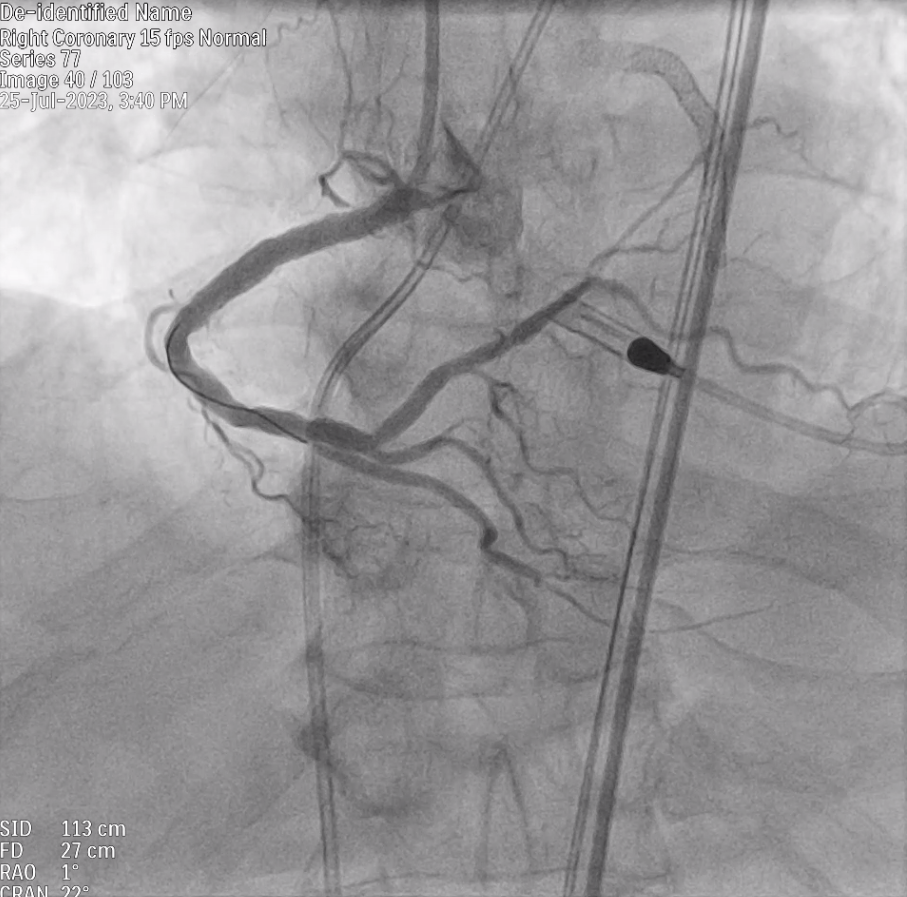
After adequate preparation, right femoral artery and vein were cannulated using 7F sheath. Through left femoral arterial approach, 5 F Pigtail catheter was taken across the aortic valve into the LV. 0.018 guide wire was placed and pigtail was then withdrawn. Over 0.018 guide wire, Impella CP was taken across the aortic valve and was positioned and initiated. The strut of prior RCA stent was protruding into aorta(10 mm). With the support of microcatheter, Whisper wire (Boston Scientific) was intentionally wired through the stent strut and the protruding segment was crushed away from the ostial RCA so as not to damage aortic valve . Serial balloon dilation was done using 1.5 , 3.0 balloons. Post Balloon dilatation, IVUS study showed minimal stent area - 10.66 mm2. Further predilatation was done using 4 x 10 mm OPN balloon ( 50 atm ), 4.5 balloons. Repeat IVUS done showed minimal stent area-16.7 mm square. Significant overlap of prior 2 stents were noted in proximal RCA in IVUS, hence third stent was avoided to prevent future ISR, hence DCB strategy was used. Using Doc Guide wire extension (Abbott Vascular) , successful PCI was done to proximal RCA using 5x 120 mm Sirolimus drug coated balloon.Final IVUS showed minimal stent area 17.72 mm2 . Impella showed transient ventriculoarterial uncoupling, suggestive of significant intra-procedure hemodynamic instability. He was slowy weaned off Impella and Impella was removed after 6 hours.
Case Summary
This case is presented as it proves the value of Impella's support for a high risk complex coronary intervention, especially in the background of cardiogenic shock and severe LV systolic dysfunction. This gentleman was discharged in 2 days and at follow-up, LV systolic function has improved and he is doing well without any complications . In high risk interventions, Impella seems to provide solid support by LV unloading and better circulation.