
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-092
Left Main Coronary Artery Total Occlusion in Recent Myocardial Infarction
By Ta-Hsin Tai, Guang-Yuan Mar, Feng Yu Kuo
Presenter
Ta-Hsin Tai
Authors
Ta-Hsin Tai1, Guang-Yuan Mar2, Feng Yu Kuo2
Affiliation
Kaohsiung Municipal United Hospital, Taiwan1, Kaohsiung Veterans General Hospital, Taiwan2,
View Study Report
TCTAP C-092
Coronary - Complex PCI - Left main
Left Main Coronary Artery Total Occlusion in Recent Myocardial Infarction
Ta-Hsin Tai1, Guang-Yuan Mar2, Feng Yu Kuo2
Kaohsiung Municipal United Hospital, Taiwan1, Kaohsiung Veterans General Hospital, Taiwan2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 70-year-old male suffered from orthopnea and exertional dyspnea for two weeks. He also mentioned about one episode of chest pain and tightness with cold sweating during the night two weeks ago. However, the patient had no other discomfort with easy looking at this moment. He was not pay much attention to it, till his son brought to our CV OPD.
Relevant Test Results Prior to Catheterization
CXR showed bilateral pleural effusion. EKG was ST elevation at V1-V3. Echocardiography showed severe hypoknesia with moderate MR.


Relevant Catheterization Findings
Left main coronary artery : total occlusion Right coronary artery middle part: 70% stenosisCollateral flow from RCA-PLV to LAD-D1
Interventional Management
Procedural Step
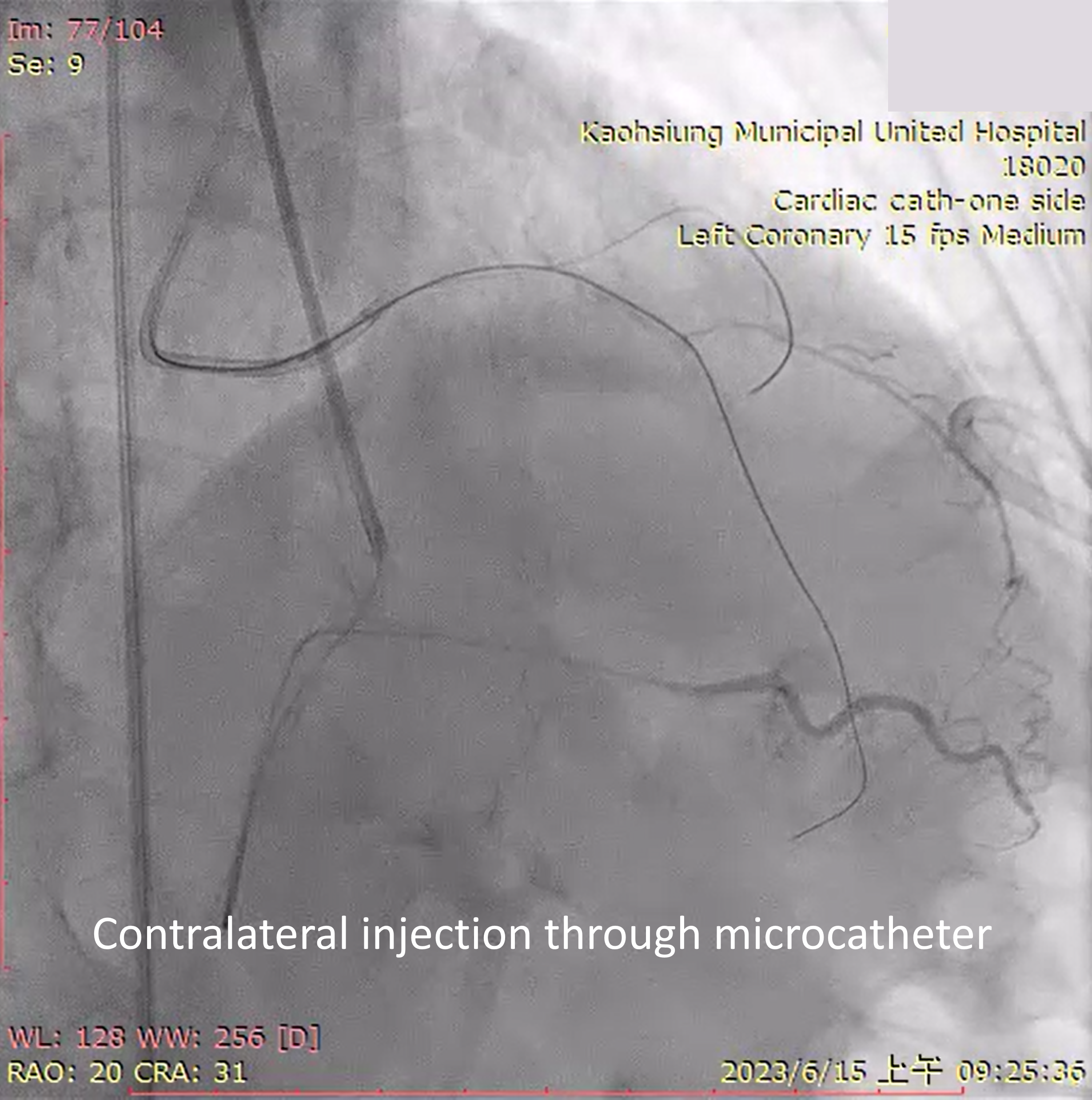
1. Left coronary artery was engaged with JL 6Fr.. Right coronary artery was engaged with JR 6Fr.2. RCA was passed with Runthrough wire, then we put a microcatheter at RCA-PLV3. Contralateral injection through microcatheter to reduce the amount of contrast, because of the poor LV function4. LM to LCX was passed with Runthrough wire through microcatheter5. LM to LAD was passed with XTA wire through microcatheter6. Contralateral injection showed wire in the true lumen7. Predilated with 1.0, 1.5, 2.0 balloon 8. IVUS was performed 9. One DES (2.5x38) was depolyed over LAD-M to LAD-D 10. One DES (3.0x38) was depolyed over LAD-P to LAD-M 11. One DES (3.5x15) was depolyed over LM to LAD-P 12. LAD-M post dilated with 2.75 NC balloon13. LM and LAD-P was post dilated with 3.5 NC balloon 14. Left coronary artery final TIMI III flow15. One DES (3.5x24) was depolyed over RCA-M 16. Final vital sign was stable without other discomfort
Case Summary
This is a 70-year-old patient with left main coronary total occlusion and recent myocardial infarction. Due to his poor LV systolic function, we use contralateral injection through microcatheter. Then IVUS gulid PCI. Three DES were depolyed over LM to LAD-D. The procedure was done smoothly. When dealing with CHIP (complex high-risk and indicated PCI) patient , we must be careful the contrast amount and surgical time. Might consider mechical support if needed.