
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-105
A Twist in the Story: Iatrogenic Catheter-Induced Coronary Artery Dissection
By Chi Tung Chen
Presenter
Chi Tung Chen
Authors
Chi Tung Chen1
Affiliation
China Medical University Hospital, Taiwan, Taiwan1,
View Study Report
TCTAP C-105
Coronary - Complication Management
A Twist in the Story: Iatrogenic Catheter-Induced Coronary Artery Dissection
Chi Tung Chen1
China Medical University Hospital, Taiwan, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 79-year-old woman arrived with a complaint of chest pain persisting for several hours. She has a history of hypertension, well-controlled with medication, and is a non-smoker. There is no notable cardiac risk in her family history. Upon cardiovascular examination, no abnormalities were detected, and her vital signs remained stable during triage.
Relevant Test Results Prior to Catheterization
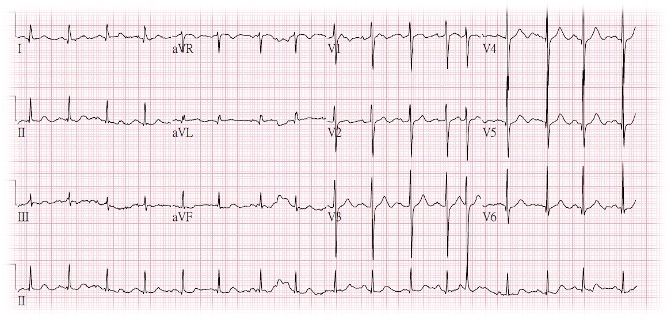
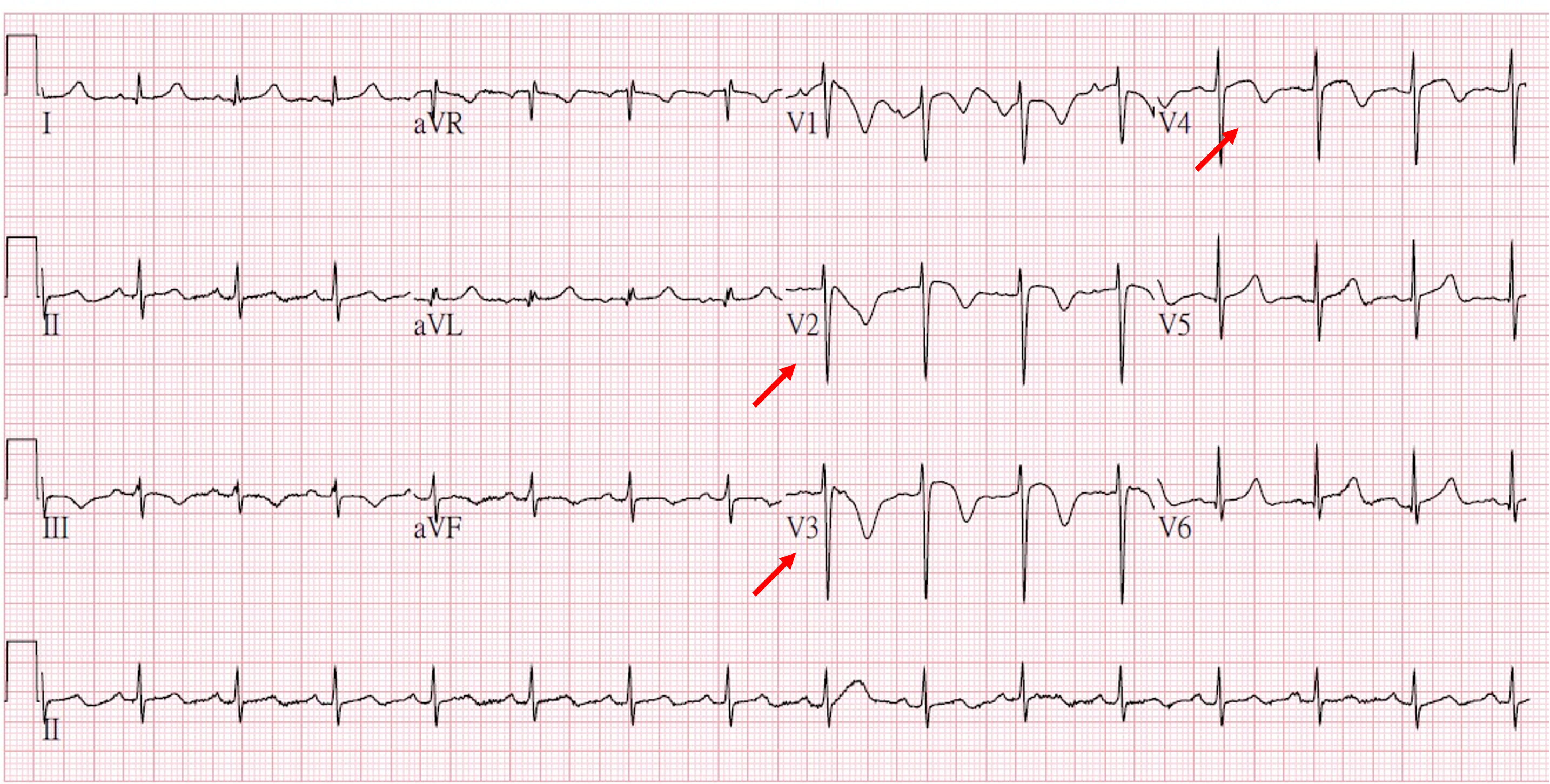
The initial electrocardiogram (ECG) displayed inverted T-waves in leads V2, V3, and V4. Compared to the previous ECG, a notable change was observed with T-wave inversion. The chest X-ray also indicated cardiomegaly with mild pulmonary congestion. Due to ongoing symptoms and the findings on the ECG, an emergent coronary angiography was performed.

Relevant Catheterization Findings
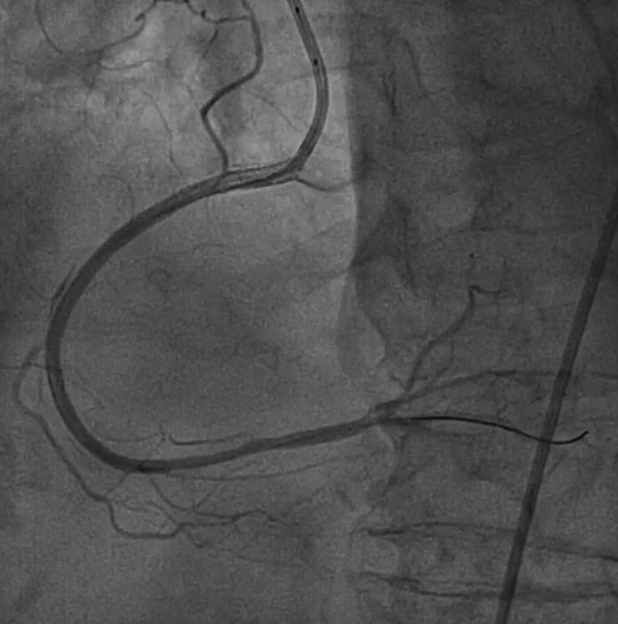
Suspecting the LCA as the potential culprit, a diagnostic approach began on the RCA. Utilizing a 6 Fr. sheath, we assessed the right femoral artery and proceeded with diagnostic catheter. Initial angiography revealed insignificant CAD with TIMI-3 flow at this stage of evaluation. However, the fluoroscopy in our cath lab experienced a temporary shutdown for one minute. A spiral dissection spanning from the ostial to distal became apparent. More, a hematoma severely comprised distal portion of RCA.

Interventional Management
Procedural Step
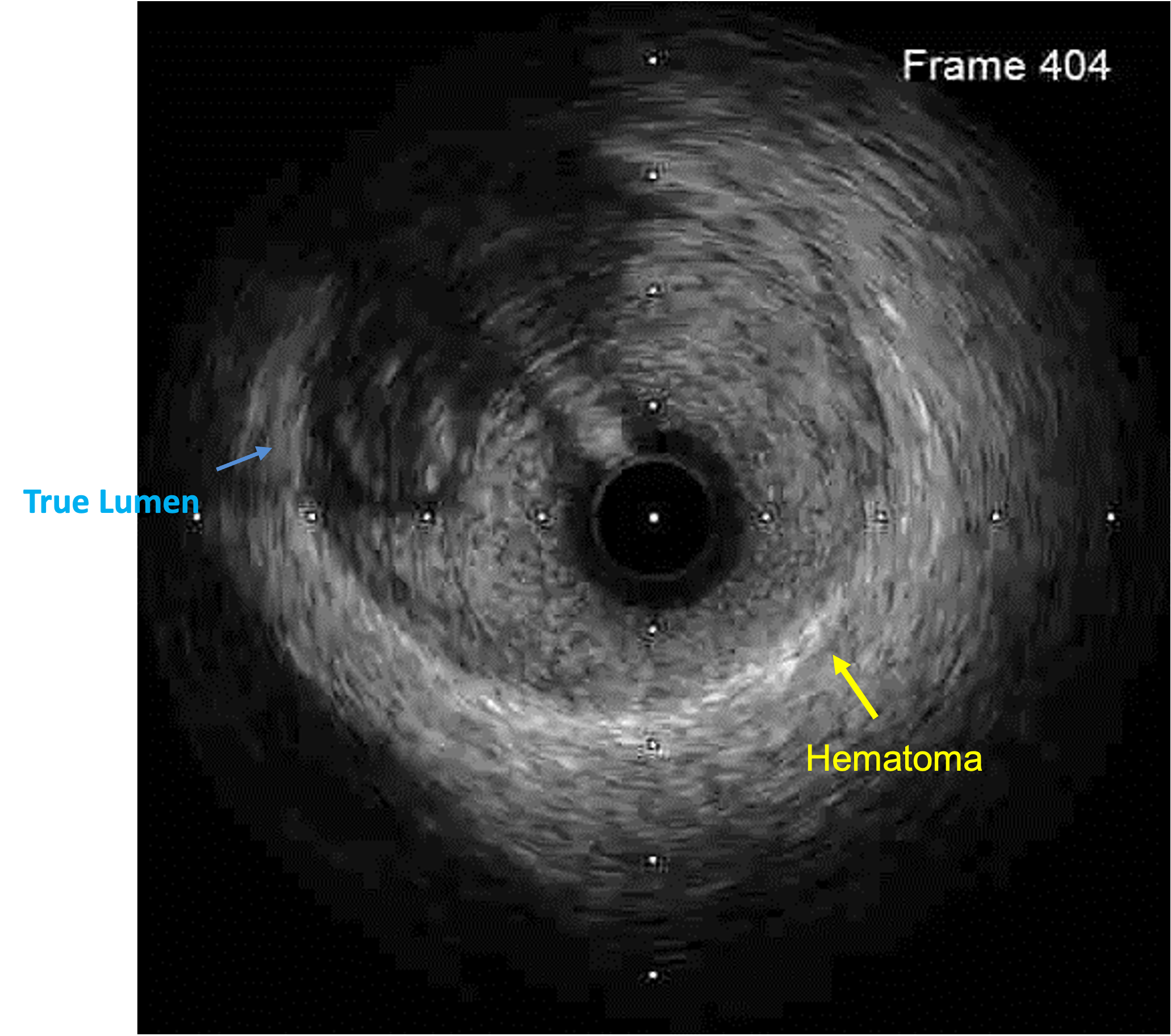
In response to the compromised RCA, we switched to a 6 Fr. JR 4 guiding catheter, positioning its tip slightly beyond the RCA ostium. Attempting to re-wire with a Sion wire revealed resistance, indicating in the false lumen. As the patient experienced bradycardia, hypotension, and desaturation, emergent intubation was performed, and the ECMO team was called. IVUS guided us to a dissection-free zone at the os-RCA. After adjusting the catheter position, we successfully re-wired with another Sion wire, confirmed in the true lumen. Serial bare metal stenting promptly secured the artery. Post-dilation and IVUS verification revealed no residual dissection at the proximal portion, which was fully covered with stents. Fortunately, TIMI 3 flow was restored, and the left coronary artery showed no critical stenosis, culminating in a satisfactory outcome.

Case Summary
Incidence of catheter-induced coronary artery dissection is estimated <0.1%, with over 50% of cases involving RCA injury. Technical factors include catheter type, position, and deep intubation. Fortunately, most patients (94.1%) safely discharged with appropriate management. Soft workhorse guidewires with a low tip load are preferred for crossing the dissected segment. IVUS proves invaluable, visualizing the entry point, confirming wire placement in the true lumen, and providing details on dissection length and vessel diameter for stenting. A common strategy involves stenting from the entry point to an area of normal vessel, effectively sealing the dissection and compressing any hematoma.