
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-157
When Drug Is Not Enough and When Enough Is Enough?
By Si Ling Soh, Aslannif Roslan, Jassie Teo, Huzairi Sani, Abdul Ariff, Shaiful Azmi Yahaya
Presenter
Si Ling Soh
Authors
Si Ling Soh1, Aslannif Roslan2, Jassie Teo2, Huzairi Sani3, Abdul Ariff2, Shaiful Azmi Yahaya2
Affiliation
National Heart Institute, Malaysia, Malaysia1, National Heart Institute, Malaysia2, Hospital Pantai Klang, Malaysia3,
View Study Report
TCTAP C-157
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
When Drug Is Not Enough and When Enough Is Enough?
Si Ling Soh1, Aslannif Roslan2, Jassie Teo2, Huzairi Sani3, Abdul Ariff2, Shaiful Azmi Yahaya2
National Heart Institute, Malaysia, Malaysia1, National Heart Institute, Malaysia2, Hospital Pantai Klang, Malaysia3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
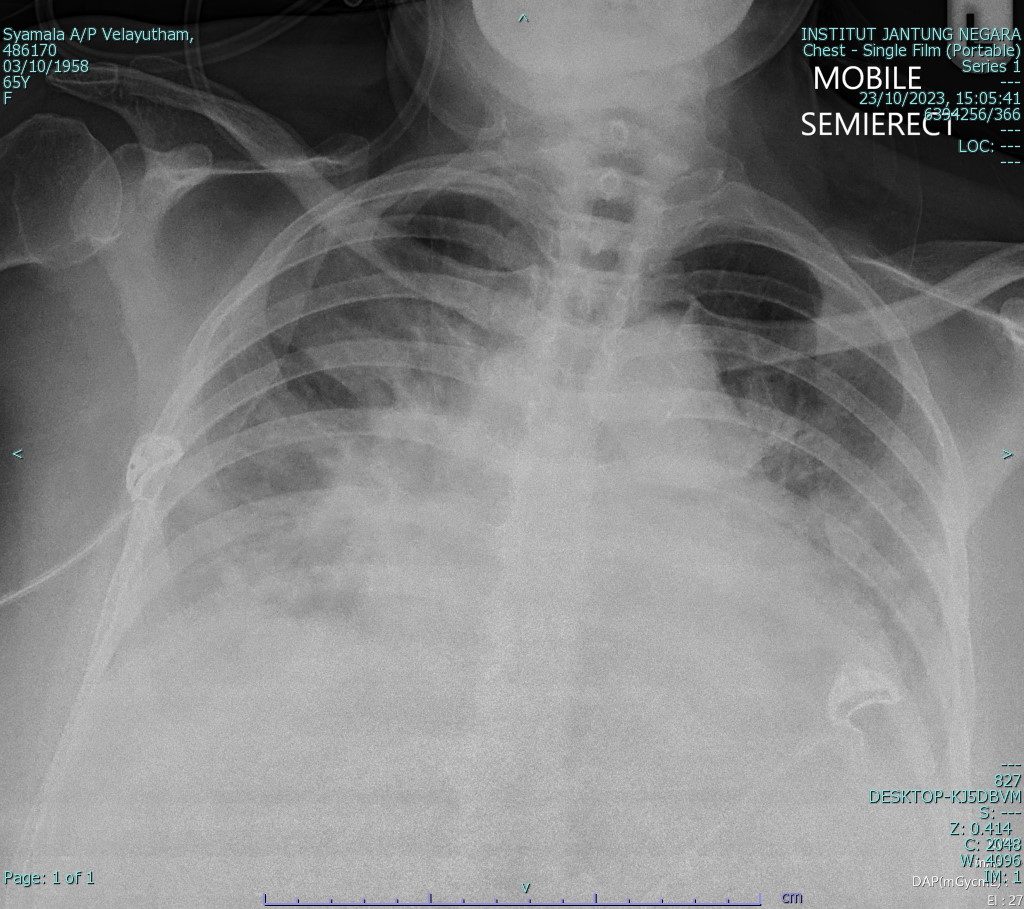
65 years old lady presented to OSH with anterior STEMI. There angioplasty was done to the totally occluded LAD with drug eluting balloon but with poor distal flow. She presented again to our center with dyspnea needing intubation and ventilation. Examination reveals lung crepitation and elevated JVP. Bedside echo shows EF of 20%. Patient develop recurrent VT and we decided to go for re-study angiogram.


Relevant Test Results Prior to Catheterization
ECG reveals T inversion of the anterior leads. Hs troponin goes from 241 to 321 and NTproBNP is 20000. CXR reveals bilateral lung congestion

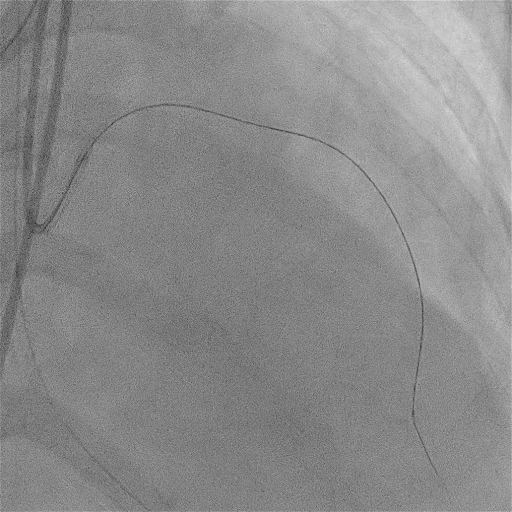
Relevant Catheterization Findings
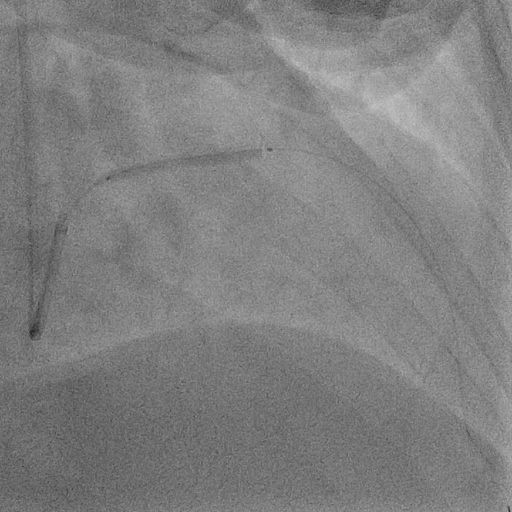
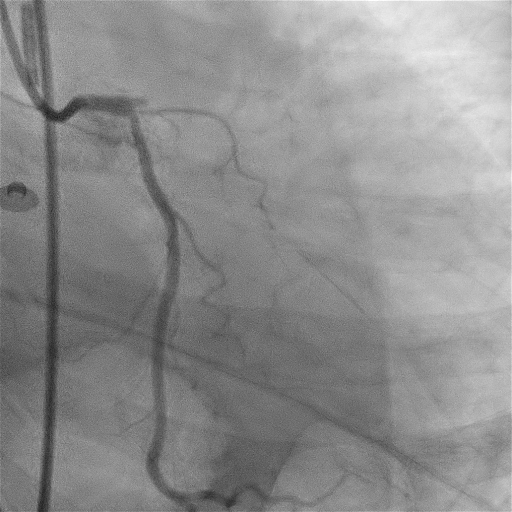
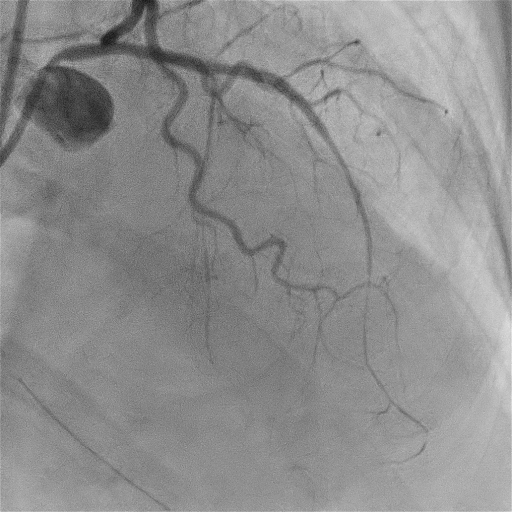
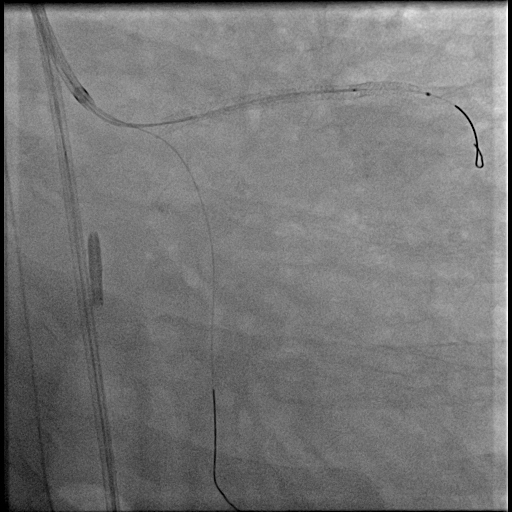
1st restudy reveals totally occluded LAD again. Decided to open it, but need stiff wire and microcatheter to cross the lesion. Ballooning causes hypotensive episodes so we quickly establish flow and stented up to LAD ostium. The result shows good distal flow. Patient still have recurrent VT afterward and we go for another restudy. Notice that the ostium of LM is diseases with pressure drop upon engagement. Quickly stent ostial LM to LCx with good result.

Interventional Management
Procedural Step
For the 1st restudy the aim is to restore flow as quickly as possible as ballooning causes hypotensive episodes and EF is poor. At 1st we though the occlusion is new so we try to cross with soft wire with balloon support but was unsuccessful. Able to cross by using stiff wire with microcatheter. To make the procedure simple and fast we decided to stent only up to LAD ostium. Able to establish good flow but noted distal stent dissection. Direct stent of the dissection was done with good final result. Unfortunately patient still having recurrent VT which we were unsure whether scar or ischemic driven. Decided to restudy again. This time we notice that the pressure damp upon EBU catheter engagement and the LM ostium is diseased. Direct stenting from ostial LM to LCx was done with good result. The LAD stent was well apposed using IVUS and we ensure also that the LM-LCx stent is properly placed also using IVUS. We decided to also do angioplasty to ostium of right coronary artery. Final result was good.

Case Summary
This case show the importance of establishing flow during the STEMI episode and whether DEB is the correct choice. As the patient presented to us one month later with poor EF and recurrent VT, its difficult to ascertain whether this is ischemia or scar driven. During 1st restudy the decision to only stent up to ostial LAD is to establish flow as quickly as possible. The ostium LM does appear diseased but as flow is established we decided to left it. However patient still have VT and we decided to go for 2nd restudy and this time directly stent ostial LM to LCx and also do the RCA. Few hours after the procedure the patient still succumb begging the question whether VT is scar driven all along