
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-194
A Challenging Case Report: Hemostasis of Right Subclavian Artery and Vertebral Artery Secondary to Artery Trauma During Central Venous Catheter Insertion
By Su-Huan Chang, Ying-Hsien Chen
Presenter
Su-Huan Chang
Authors
Su-Huan Chang1, Ying-Hsien Chen1
Affiliation
National Taiwan University Hospital, Taiwan1,
View Study Report
TCTAP C-194
Endovascular - Other Endovascular Intervention
A Challenging Case Report: Hemostasis of Right Subclavian Artery and Vertebral Artery Secondary to Artery Trauma During Central Venous Catheter Insertion
Su-Huan Chang1, Ying-Hsien Chen1
National Taiwan University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
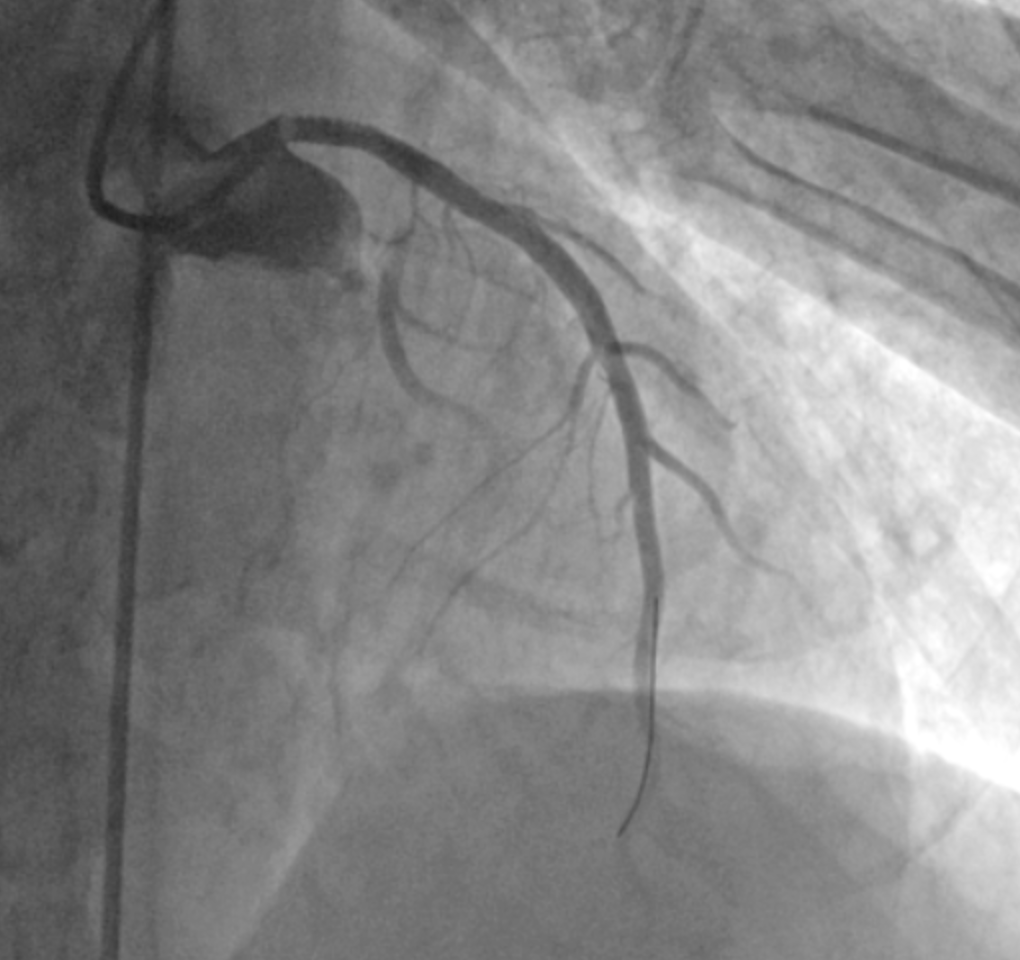
The 62-year-old male patient suffered from sudden onset chest pain since morning. ECG showed precordial leads ST elevation, which anteroseptal wall STEMI was diagnosed. Coronary angiography showed LMCA thrombus and suction was performed. A DES was deployed from LMCA to proximal LAD. A central venous catheter was inserted at right internal jugular vein for inotropes. However, right neck ecchymosis, hematoma and hypotension were developed. Accidental trauma of right neck artery was suspected.


Relevant Test Results Prior to Catheterization
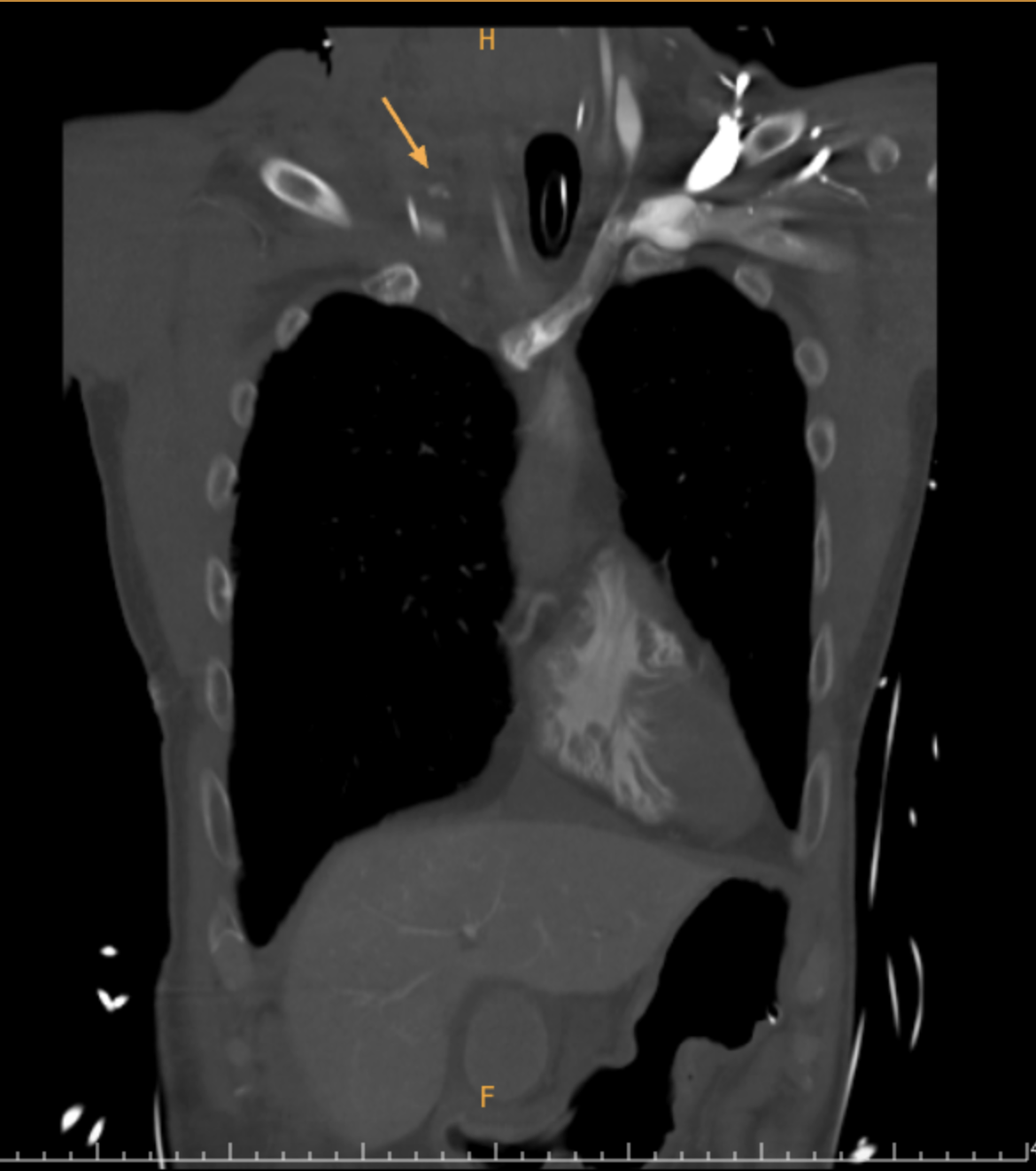
A chest plain film was performed and the result showed right lung totally white out. A CT angiography was performed for identifying the bleeding site and the result showed massive right hemothorax, active extravasation from proximal subclavian and vertebral arteries. Lab data showed Hb: 12.1g/dL, PLT 197u/kL, Fibrinogen 105.0mg/dL, and lactate 8.4mmol/L. An endotracheal tube was inserted for protecting the airway. A right lung chest tube was also placed for hemothorax treatment.

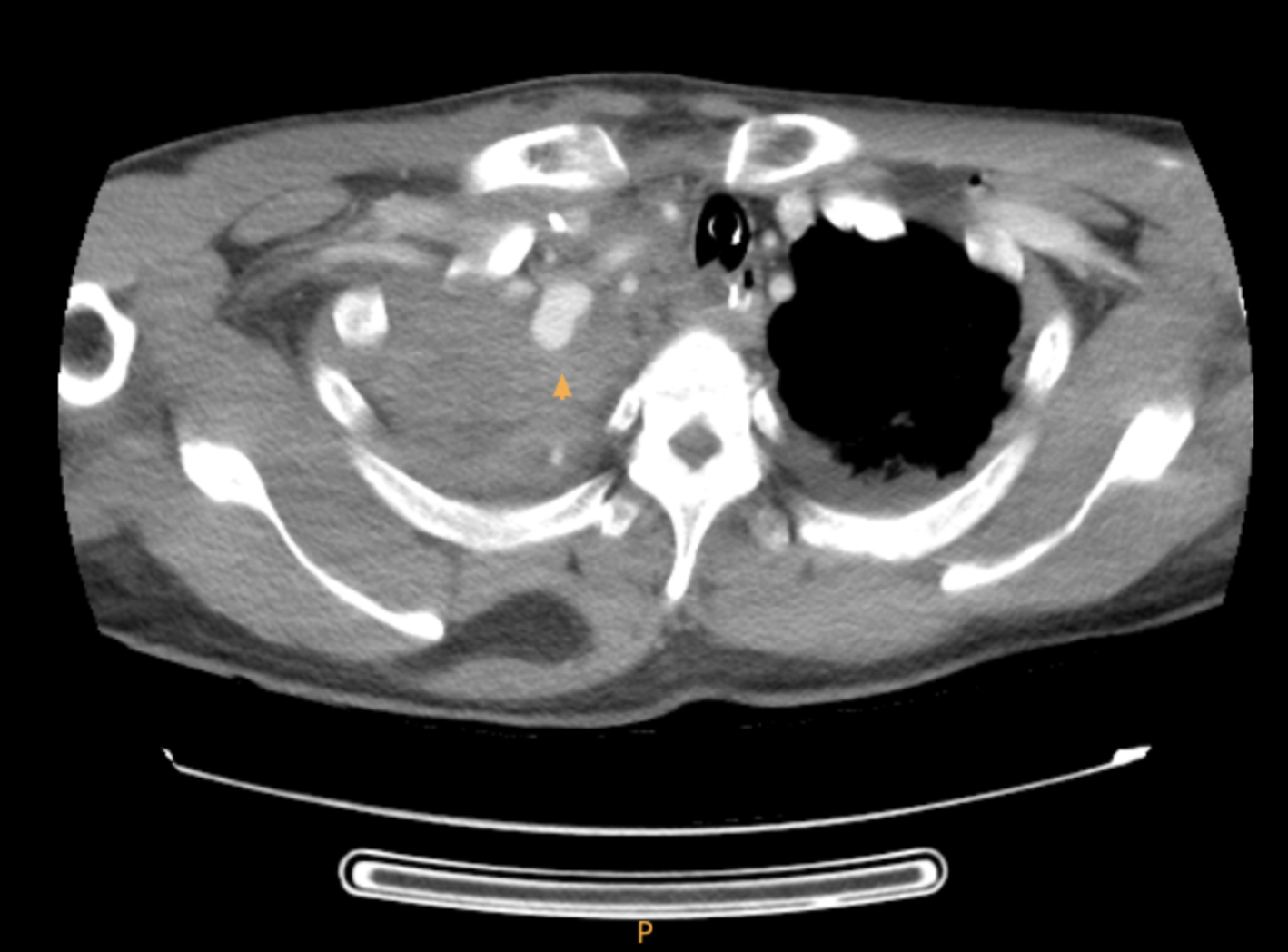
 CTA of right subclavian artery extravasation.png
CTA of right subclavian artery extravasation.png
Relevant Catheterization Findings
Right radial artery was punctured for the intervention access. Right innominate artery angiography was performed and the result revealed extravasation from proximal subclavian artery with pseudo-aneurysm formation, and proximal vertebral artery extravasation.
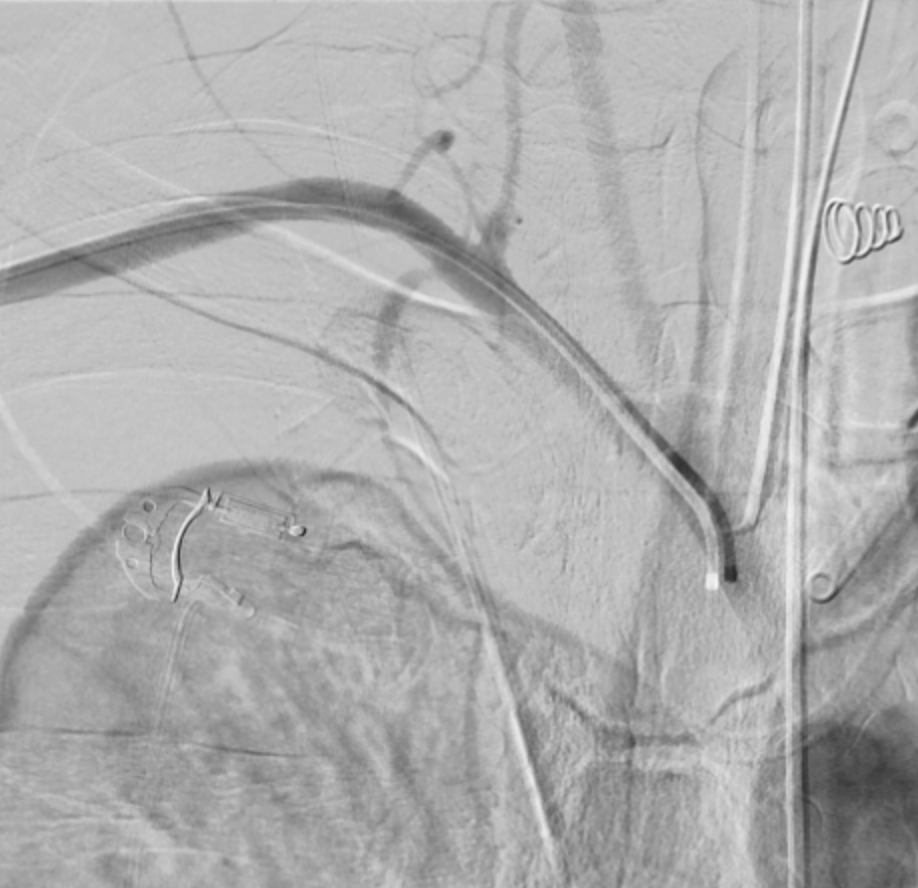
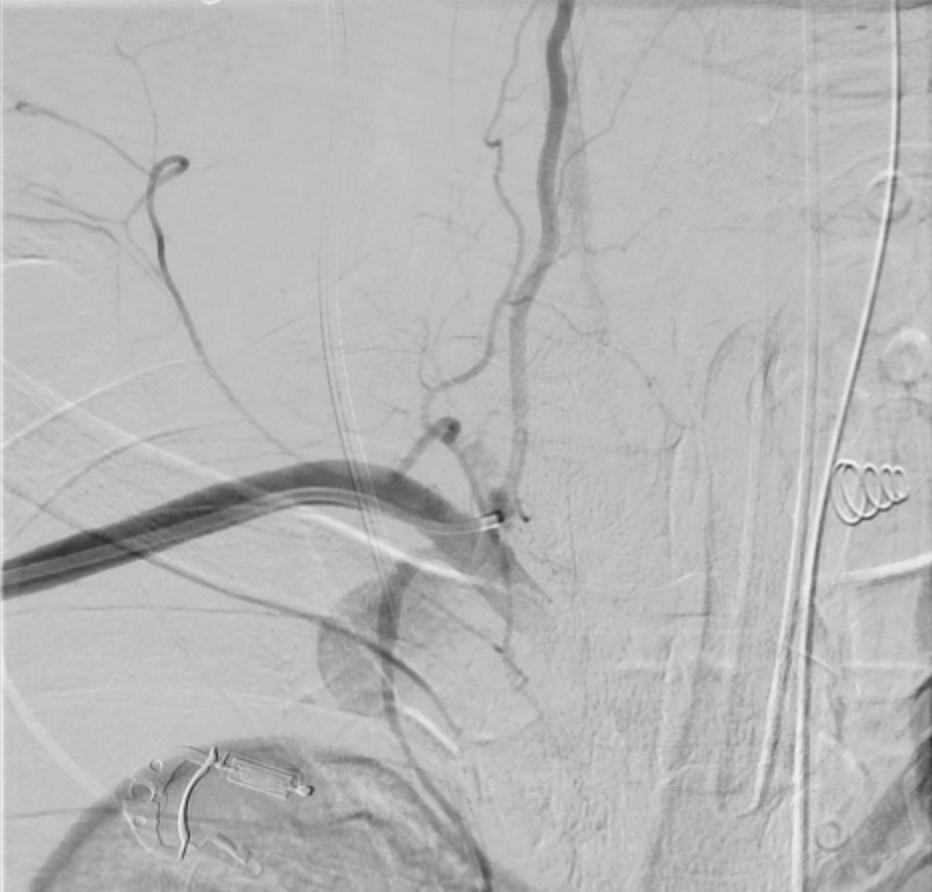

Rt subclavian artery extravasation with pseudoaneurysm and vetebral artery extravasation.png
Interventional Management
Procedural Step
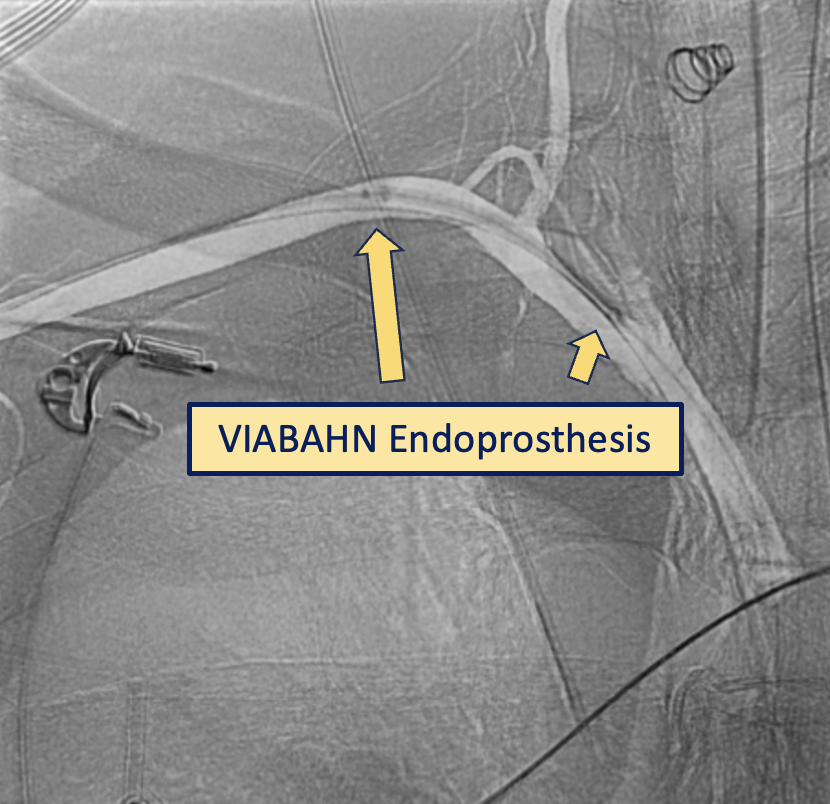
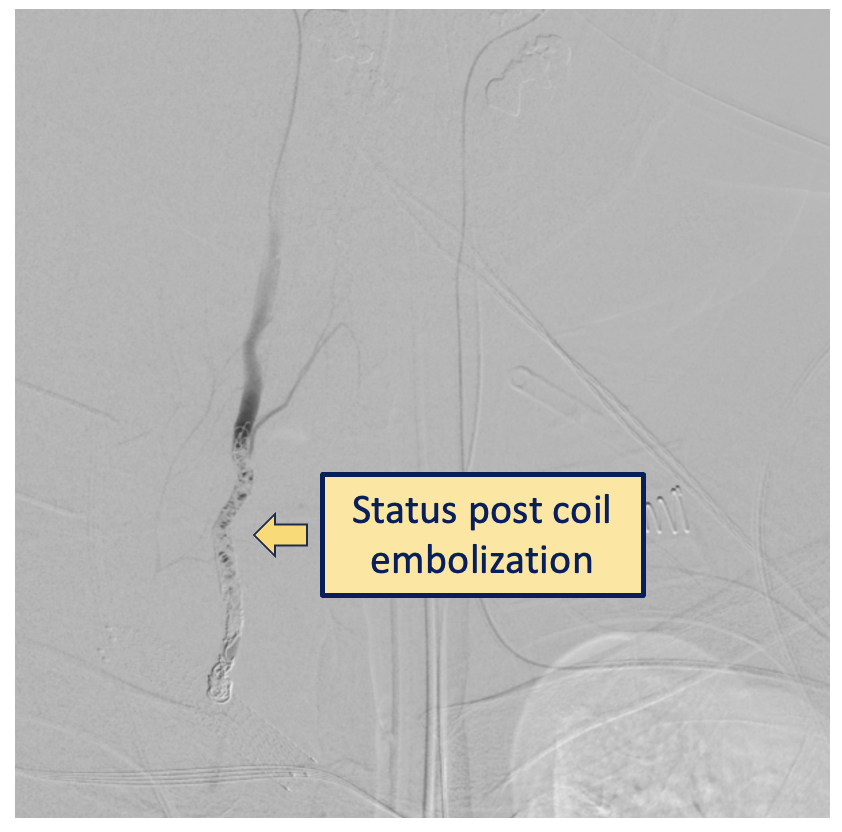
We engaged to right subclavian artery with Medtronic JR4 6Fr guiding catheter and wired to vertebral artery with ASAHI Sion wire from right radial artery access. We then performed balloon tamponade for hemostasis using Terumo Ryurei PTCA balloon 2.5*15mm and 3.0*15mm at proximal vertebral artery. Deployed BIOTRONIK PK Papyrus Covered Stent 3.0*20mm from the ostium of the vertebral artery. However, extravasation only improved partially and bleeding was still noted at the junction of the subclavian artery and vertebral artery. We then deployed GORE VIABAHN Endoprosthesis 8mm*50mm retrogradely from the proximal of right subclavian artery and crossing the vertebral artery. Final angiography showed no extravasation but jailed of the vertebral artery. However, the amount of the chest tube didn't decrease after the procedure. We then repeated CT angiography and found there was still extravasation noted at right subclavian artery, which suspecting endoleak. We punctured left radial artery for another vascular access and wired to right vertebral artery through the vertebrobasilar junction. The angiography showed bleeders at the right vertebral artery to subclavian artery junction. We advanced a microguidewire microcatheter set through the vertebrobasilar junction to the right vertebral artery orifice. We embolized the right vertebral artery with multiple pushable coils. The final angiography showed minimal extravasation. Under component therapy, the bleeding was controlled.
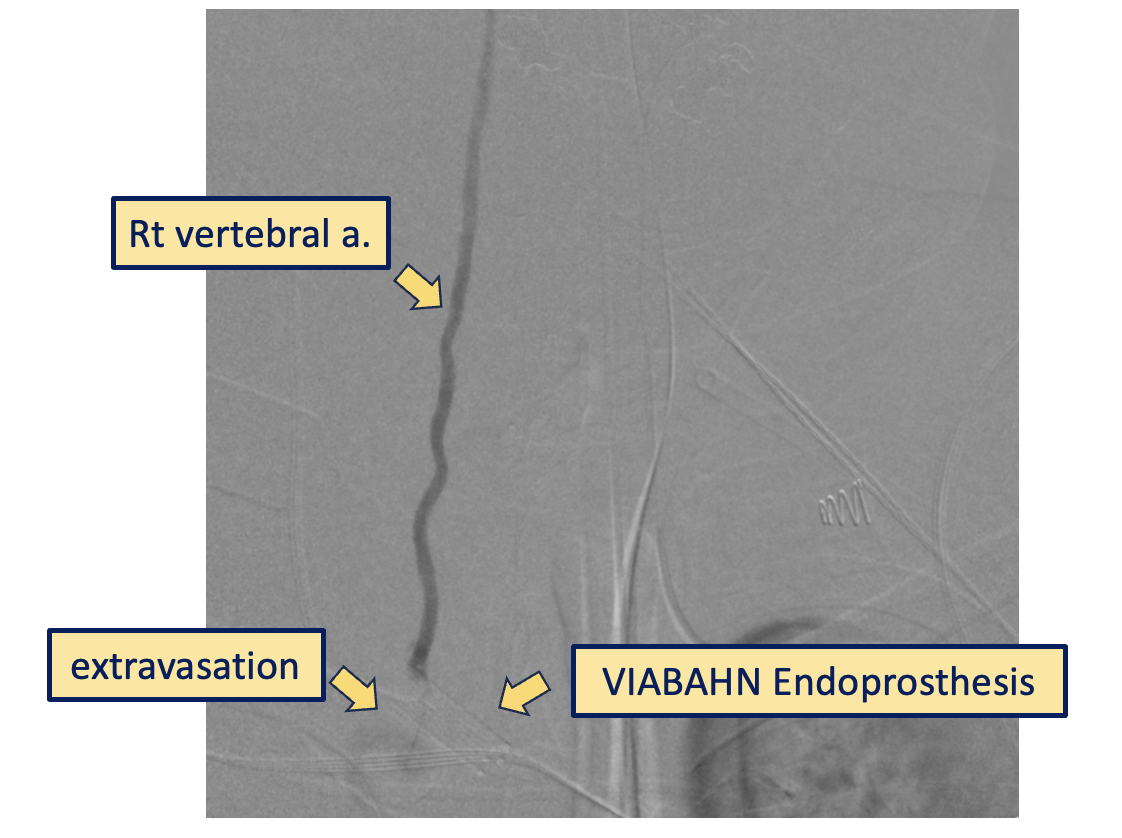
Rt vertebral artery extravasation at the junction of subclavian and vertebral a..png
Case Summary
This 62-year-old male patient suffered from right massive hemothorax owing to right subclavian artery and vertebral artery extravasation during right neck CVC insertion. Initial endovascular hemostasis was performed with cover stent to right vertebral artery and right subclavian artery . Bleeding was attenuated, but remained insufficient. Additional Coil embolization through left vertebral artery across vertebrobasilar junction and into right vertebral artery finally achieved the best hemostasis.