
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-216
A Good Plan in Succeeding a Way Out
By Kar Lok Leo Lai, Ka Lung Chui, Kevin Ka-Ho Kam, Simon Chow, Albert Kam Ming Chan, Randolph Hung-Leung Wong, Kent, Chak Yu So
Presenter
Kar Lok Leo Lai
Authors
Kar Lok Leo Lai1, Ka Lung Chui1, Kevin Ka-Ho Kam1, Simon Chow1, Albert Kam Ming Chan2, Randolph Hung-Leung Wong1, Kent, Chak Yu So3
Affiliation
Prince of Wales Hospital, Hong Kong, China1, Prince of Wales Hospital, Hong Kong, China, Hong Kong, China2, Prince Of Wales Hospital, Chinese University of Hong Kong, Hong Kong, China3,
View Study Report
TCTAP C-216
Structural - Mitral Valve Intervention - Transcatheter MV Replacement
A Good Plan in Succeeding a Way Out
Kar Lok Leo Lai1, Ka Lung Chui1, Kevin Ka-Ho Kam1, Simon Chow1, Albert Kam Ming Chan2, Randolph Hung-Leung Wong1, Kent, Chak Yu So3
Prince of Wales Hospital, Hong Kong, China1, Prince of Wales Hospital, Hong Kong, China, Hong Kong, China2, Prince Of Wales Hospital, Chinese University of Hong Kong, Hong Kong, China3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
An 83 year old lady presented with NYHA III symptoms. She had a background of mitral valve repair with Seguin Annuloplasty Ring size 28 for severe mitral regurgitation due to ruptured chordae at P2/P3 segment. Her other past medical history included diabetes mellitus , atrial fibrillation on warfarin and hypertension.

Relevant Test Results Prior to Catheterization
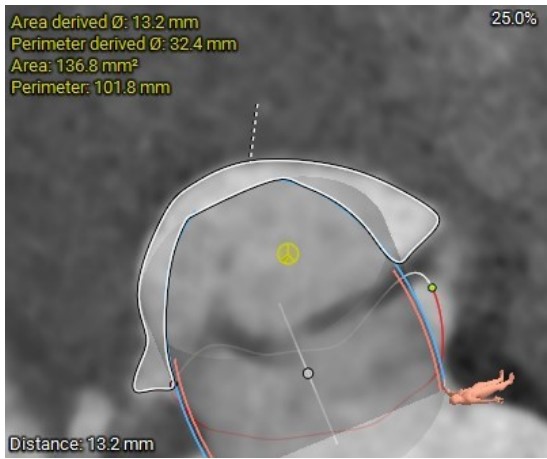
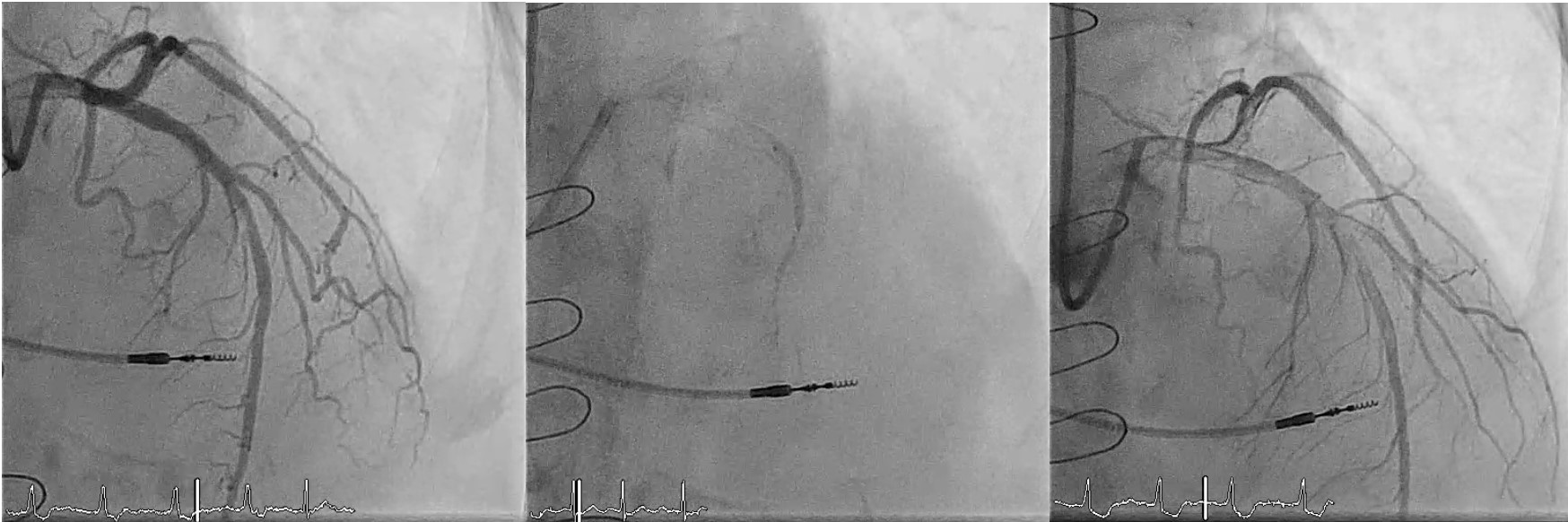
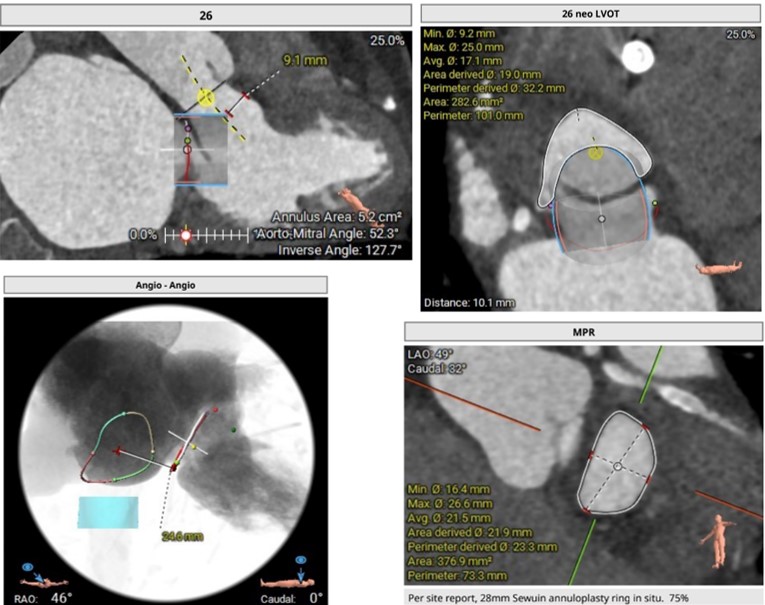
Blood tests showed NTProBNP of 3629. ECG showed AF with QRS 92ms. Transthoracic echocardiogram showed LVEF of 56%, P2 prolapse with ruptured MV chordae with flail posterior leaflet. There was severe eccentric MR, mean trans-mitral gradient of 6.5mmHg. Coronary angiogram showed mild CAD. Her STS mortality score for MVR was 12%. Heart Team concluded that patient was deem surgically inoperable and suggested for TMVR. CT analysis showed NeoLVOT area of only 135mm^2 and a high risk of LVOTO.

Relevant Catheterization Findings
Pre-emptive alcohol septal ablation was performed. S1 distal branch was selected after sonovue mapping instead of S2. Runthrough EF inside OTC 2.0 x 15mm was used. A total of 1.5cc alcohol was injected. Post ASA resulted into complete heart block and a leadless pacemaker was inserted. After 4 weeks, repeated CT showed adequate NeoLVOT area of 282mm^2, and hence decided to proceed for TMVR. Also the ring was radiolucent, there was no fluoroscopic marker, and so additional measures were required.

Interventional Management
Procedural Step
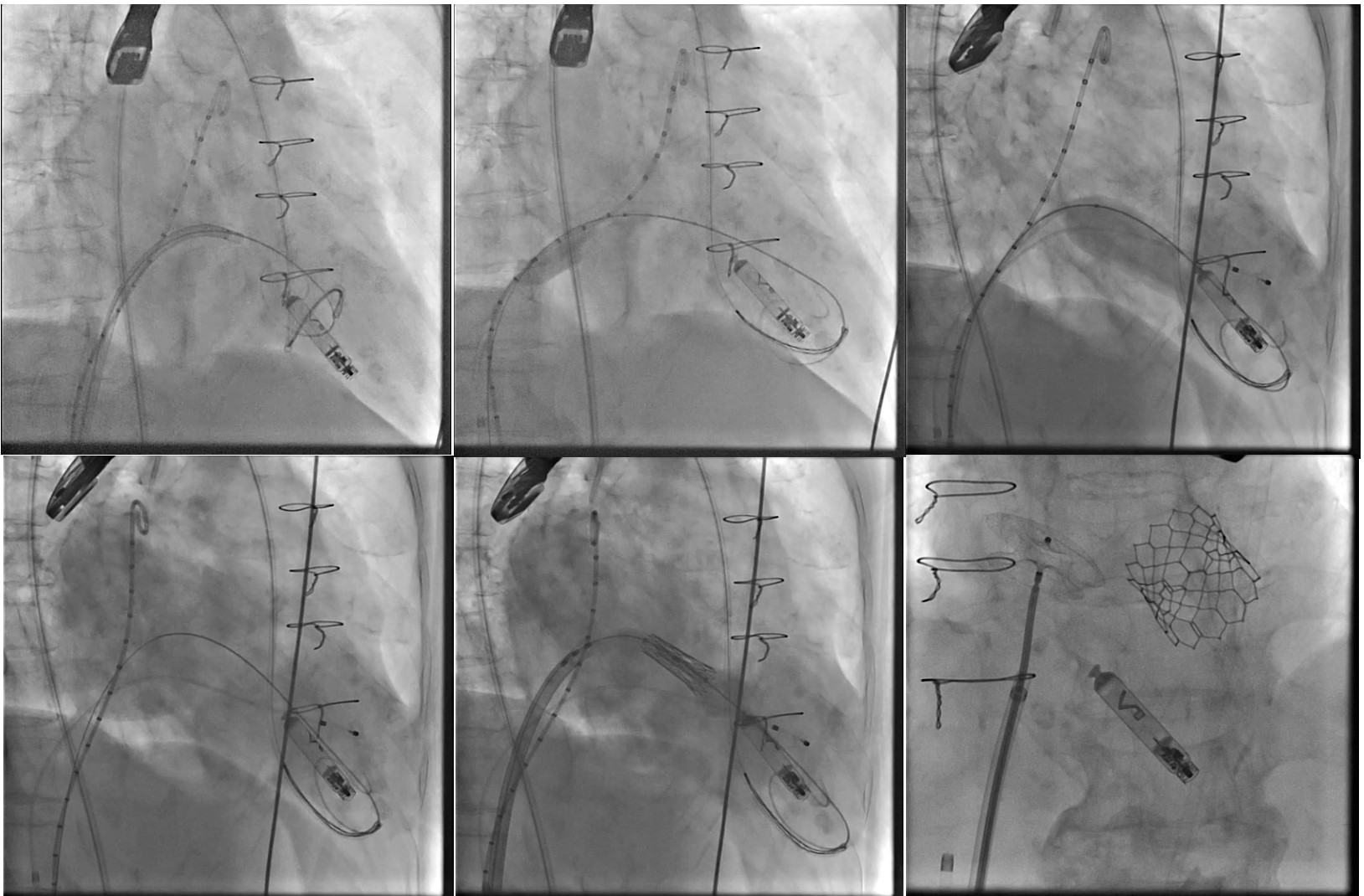
We obtained the transeptal access at height 3.7cm, inferior-posterior under TEE guidance using SL1, BRK-1 needle. Then exchanged to a super-stiff wire and a long J wire to insert a 5Fr pigtail for LA angiogram, then inserted the 14Fr E sheath, and followed by a medium curl Agilis 8.5Fr into LA. Next, we performed the LV wire snaring by inserted JL 3.5 7Fr guiding catheter through left femoral arterial access, with inside a 18-30 Ensnare inserted. Over the Agilis Sheath, a 6Fr pigtail crossed the Memo 4D mitral valve ring. The pigtail was then snared by the JL guiding catheter from arterial side, then the pigtail was exchanged to a preshaped Confida wire into left ventricle.
Balloon septostomy was then performed using a 14mmx40cm Armanda balloon. Balloon predilatation to determine the waist of the ring, LA angiogram and live biplane TEE guidance were used to guide as a roadmap for the TMVR deployment. A Sapien 26mm(+1cc) was prepared and deployed under rapid pacing at 180bpm with optimal depth (20 LA/80 LV) successfully.
Iatrogenic ASD was then closed with a 16mm Amplatzer ASD device with no residual leak.
Balloon septostomy was then performed using a 14mmx40cm Armanda balloon. Balloon predilatation to determine the waist of the ring, LA angiogram and live biplane TEE guidance were used to guide as a roadmap for the TMVR deployment. A Sapien 26mm(+1cc) was prepared and deployed under rapid pacing at 180bpm with optimal depth (20 LA/80 LV) successfully.
Iatrogenic ASD was then closed with a 16mm Amplatzer ASD device with no residual leak.
Case Summary
In conclusion, TMVR valve-in-ring procedure was safe and effective after pre-emptive ASA. An accurate pre CT planning was crucial in achieving a satisfactory outcome. Also, despite the radiolucency of the mitral ring, balloon pre-dilatation, LA angiogram and TEE guidance all gave additional insights and a road to success for the accurate TMVR deployment.