
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-071
Case Report: Sunlight After the Storm: Difficult Calcified Chronic Total Occlusion and Upfront Two Stent Strategy Bifurcation of LAD/D1 PCI
By Richard Chay Shien Long, Jin Kiang Cheng, Jian Hao Sim, Hou Tee Lu, Azrina Abdul Kadir, Gurudevan Mahadevan, Wee Pang Ng, Wen Sheng Wong, Waye Young Lau
Presenter
Richard Chay Shien Long
Authors
Richard Chay Shien Long1, Jin Kiang Cheng2, Jian Hao Sim3, Hou Tee Lu3, Azrina Abdul Kadir3, Gurudevan Mahadevan3, Wee Pang Ng3, Wen Sheng Wong3, Waye Young Lau3
Affiliation
Sultanah Aminah Hospital,, Malaysia1, Hospital Sultanah Aminah, Malaysia2, Sultanah Aminah Hospital, Malaysia3,
View Study Report
TCTAP C-071
Coronary - Complex PCI - CTO
Case Report: Sunlight After the Storm: Difficult Calcified Chronic Total Occlusion and Upfront Two Stent Strategy Bifurcation of LAD/D1 PCI
Richard Chay Shien Long1, Jin Kiang Cheng2, Jian Hao Sim3, Hou Tee Lu3, Azrina Abdul Kadir3, Gurudevan Mahadevan3, Wee Pang Ng3, Wen Sheng Wong3, Waye Young Lau3
Sultanah Aminah Hospital,, Malaysia1, Hospital Sultanah Aminah, Malaysia2, Sultanah Aminah Hospital, Malaysia3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 66 years old Indian gentleman with long standing diabetes mellitus and former cigarette smoker presented to the out patient cardiology clinic with chronic angina for 1 year. His glycemic control is good with oral hypoglycemic drugs and he has stopped smoking past 2 years. He does not have failure symptoms and is clinically not fluid overloaded. He is overweight and leads a sedentary lifestyle. Lungs were clear and there were no pedal edema. BP 132/84 mm Hg; HR 66 bpm; spO2 98% in room air;
Relevant Test Results Prior to Catheterization
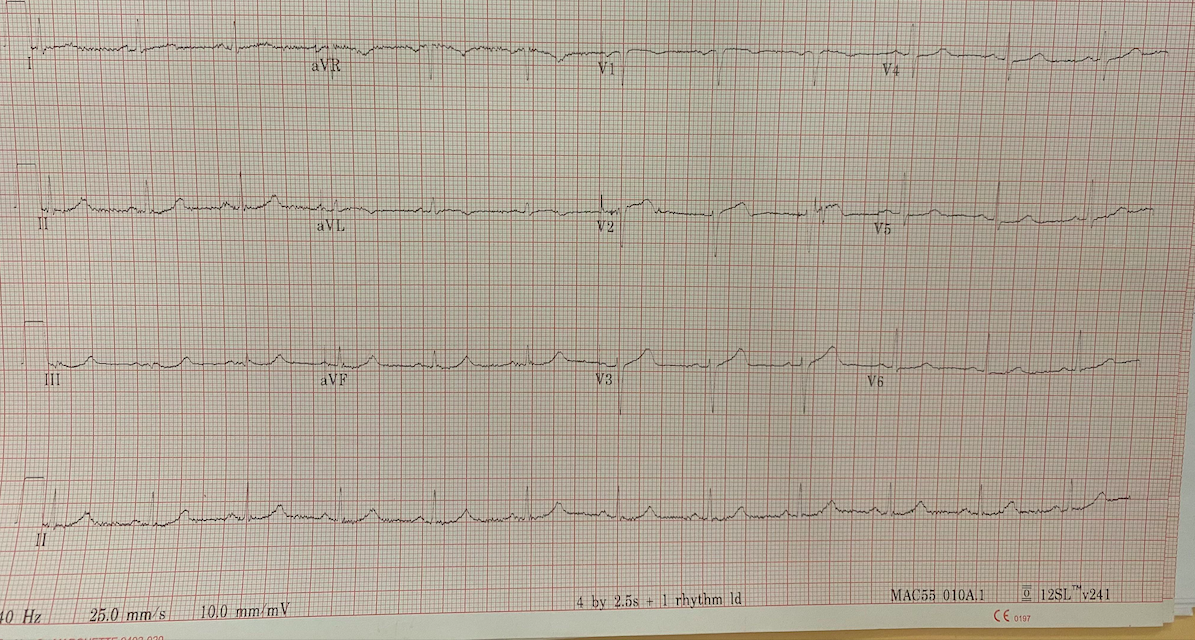
12 lead ECG: normal sinus rhythm; left axis deviation; left ventricular hypertrophy;
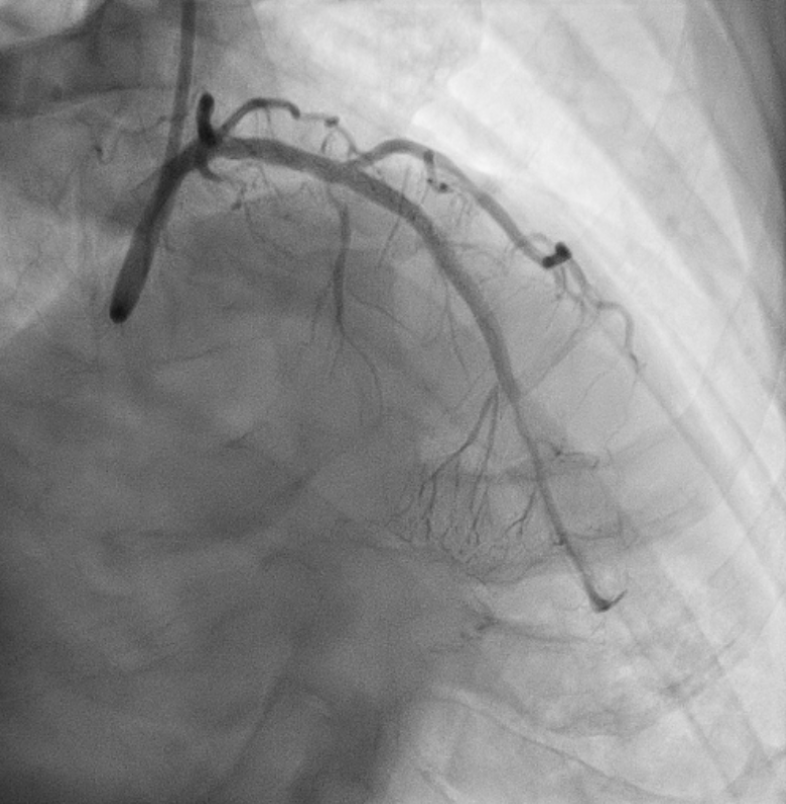
Relevant Catheterization Findings
PLAD CTO; collaterals from RCA to LAD
Interventional Management
Procedural Step
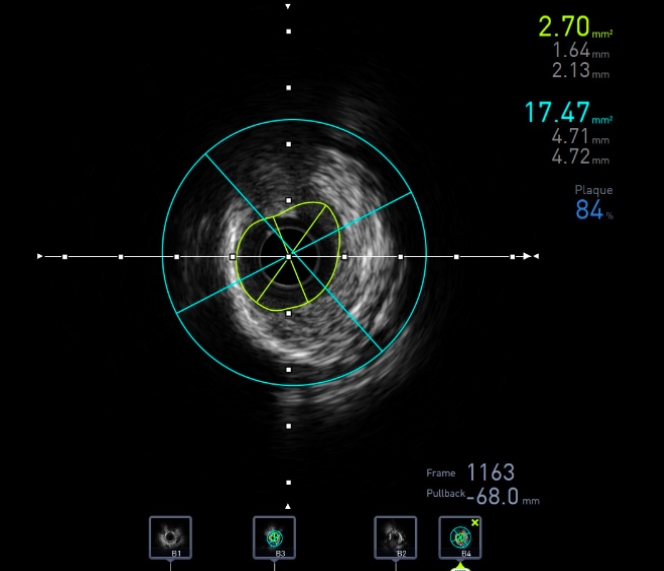
PCI to LAD via double puncture into right radial & right femoral. LCA engaged with 7F EBU 3.5 & RCA with 6F AL 0.75; Antegrade approach. Wire down LAD with Fielder XT-R through microcatheter. Wire escalation with UB3 & Gaia2 but went into false lumen. Use parallel wire technique with Conquest Pro & able to cross MLAD CTO. Distal wire tip confirm with contralateral injection. Difficult to pass small balloon beyond CTO. Had to use guide extension catheter & balloon anchoring technique to deliver balloon. MLAD CTO predilated with SC 0.85x10mm, SC 1x5mm & SC 1.25x10mm. All 3 balloons burst. Conquest Pro exchanged to Runthrough floppy. MLAD predilated with SC 2x20mm. IVUS confirm wire in true lumen, circumferential calcified lesion over PLAD & vessel size. Use scoring balloon 1.75x15mm. IVUS show calcium cracks. LAD predilated with NC 1.5x15mm & NC 3x15mm. Patient had transient bradycardia. Responded to IV atropine 0.5mg & 1 pint normal saline. We use mini crush technique for diagonal branch & PLAD. Diagonal branch predilated with SC 2x20mm before stent with Resolute Integrity 2.25x18mm. PLAD stent with Resolute Onyx 3x34mm. Kissing balloon technique. Post dilated PLAD with NC 3x15mm & NC 3.5x8mm. Rewire into side branch. KBI & POT. MLAD stent with Promus Elite 2.25x32mm. DLAD DCB with Prevail 2x30mm. IVUS show good stent expansion & apposition. Procedure time 5 hrs 30 mins. Contrast 480ml. Patient discharged well the next day.

Case Summary
This case illustrates antegrade wire escalation in a calcified CTO lesion to successful crossing. IVUS plays an important role in this case as it allows us to study the morphology and severity of the calcification and strategy for calcium modification prior to stenting, apart from confirming wire in the true lumen, estimating vessel size and stent optimization. We performed upfront 2 stent strategy as the diagonal fulfills major and some minor criteria. We opted for mini crush bifurcation technique mainly to simplify and shorten procedural time after difficult crossing and lesion preparation in the calcified LAD CTO.