
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-064
A Complicated Road Block: Left Main Coronary Artery Chronic Total Occlusion Intervention Using Nano- Crush Bifurcation Technique
By Avik Karak, Kuntal Bhattacharyya, Jayanta Saha
Presenter
Avik Karak
Authors
Avik Karak1, Kuntal Bhattacharyya2, Jayanta Saha2
Affiliation
Fortis Hospital, India1, Kolkata Medical College & Hospital, India2,
View Study Report
TCTAP C-064
Coronary - Complex PCI - CTO
A Complicated Road Block: Left Main Coronary Artery Chronic Total Occlusion Intervention Using Nano- Crush Bifurcation Technique
Avik Karak1, Kuntal Bhattacharyya2, Jayanta Saha2
Fortis Hospital, India1, Kolkata Medical College & Hospital, India2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
49 year old male smoker presented with refractory angina and Shortness of breath of class III. Well controlled hypertension. Positive family history of atherosclerotic cardiovascular disease. Symptoms worsening over the last one month. Blood pressure of 124/66 mmHg. Pulse rate of 68 beats per minute. Cardiovascular system examination unremarkable.

Relevant Test Results Prior to Catheterization
Routine blood investigations unremarkable. Normal glycemic control. LDL - 88 mg/dl. Resting electrocardiogram normal. Echocardiogram showed a normal resting LV function. Exercise stress testing was strongly positive at a very low workload.
Relevant Catheterization Findings
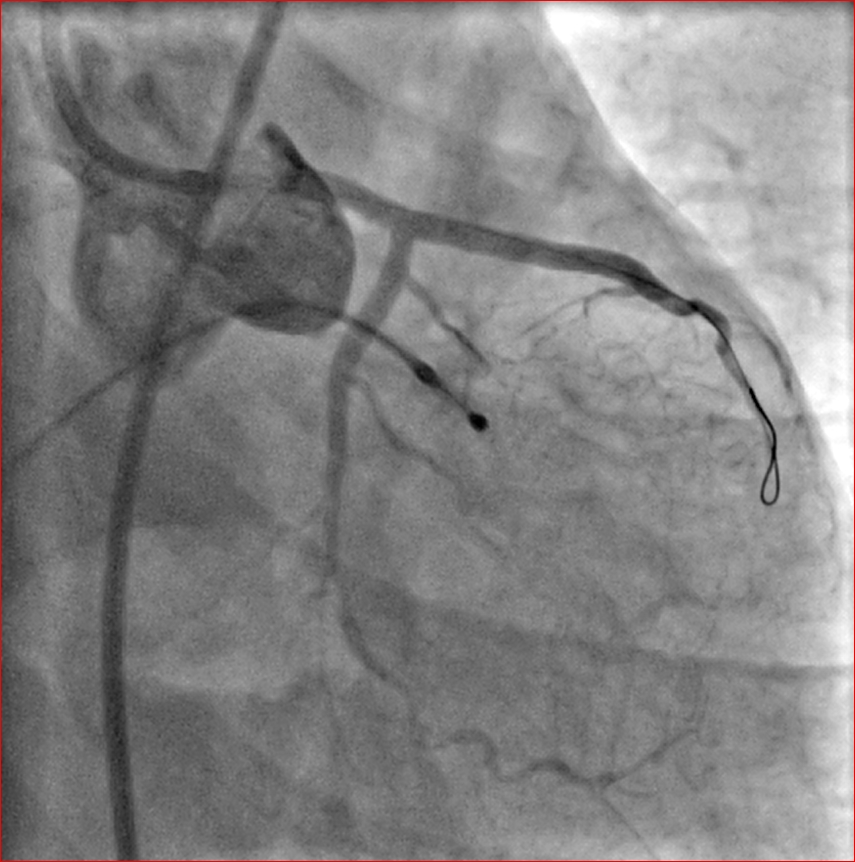
Coronary angiogram showed a chronic total occlusion of the distal left main coronary artery. Right dominant circulation. Proximal right coronary artery showed minor plaque with retrograde supply to the left anterior descending and circumflex arteries from distal right coronary artery. Left ventricular angiogram showed a normal function.



Interventional Management
Procedural Step
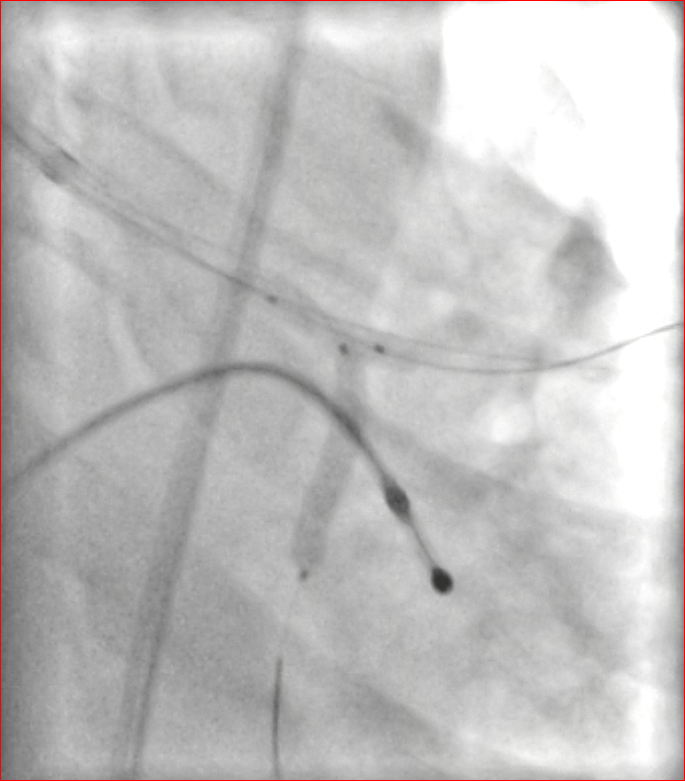
Temporary pacemaker lead was positioned in right ventricle via right femoral vein. Right femoral artery and right radial artery were cannulated. 7 Fr EBU 3.5 (Extra backup) catheter was used to intubate the LMCA. Dual injection was taken from RCA. The distal LMCA CTO segment was crossed into LCX using microcatheter and Fielder XT (Ashahi intecc, Japan) guidewire which was exchanged with Runthrough guidewire (Ashahi intecc, Japan). The proximal LAD segment was crossed with Fielder XT wire and microcatheter and the mid LAD segment was crossed using Gaia II (Ashahi intecc, Japan) guidewire with microcatheter support which was exchanged with Runthrough wire. Serial predilatation of both the LAD and LCX was done. Nano crush technique was used for LMCA bifurcation stenting. 2.75 × 24 mm stent was deployed in circumflex with a 3 × 15 mm noncompliant balloon kept inflated in LMCA across the circumflex ostium. After kissing balloon inflation, a 2.5 × 38 mm stent was deployed in the mid LAD followed by a 3 × 23 mm stent for the LMCA. Proximal optimisation (POT) was done in the LMCA with a 4 × 12 mm noncompliant balloon followed by rewiring into LCX. Final kissing balloon inflation was done with 3.5 × 12 mm and 2.5 × 12 mm noncompliant balloons in LAD and LCX respectively. Re-POT was done with the 4 mm noncompliant balloon. Intravascular ultrasound imaging was done which showed excellent stent apposition and adequate luminal area in the stented segments. Good distal TIMI III flow was achieved.

Case Summary
Coronary artery bypass grafting is recommended in such scenario but angioplasty is a feasible option if planned appropriately. Selection of the catheters and guidewires is very important. Our case was challenging because of multiple CTO segments especially difficult being the distal cap at an acute angulation in the mid LAD. Dual injection from RCA helped us in confirming the distal wire positions. Nano crush bifurcation strategy is a novel and excellent technique in such scenarios and reduces the metal burden at the neo carina. POT, final kissing balloon inflation and re-POT are essential in any bifurcation technique. Intravascular imaging (IVUS in our case) is essential in such cases.