
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-130
Recurrent Cardiac Tamponade After Rotablator-Associated Coronary Perforation Treated With Additional Covered Stent Implantation
By Koichiro Hori, Shunsuke Matsuno, Mayu Sakuma, Mikio Kishi, Hiroto Kano, Yuji Oikawa, Junji Yajima
Presenter
Koichiro Hori
Authors
Koichiro Hori1, Shunsuke Matsuno1, Mayu Sakuma1, Mikio Kishi1, Hiroto Kano1, Yuji Oikawa1, Junji Yajima1
Affiliation
The Cardiovascular Institute, Japan1,
View Study Report
TCTAP C-130
Coronary - Complication Management
Recurrent Cardiac Tamponade After Rotablator-Associated Coronary Perforation Treated With Additional Covered Stent Implantation
Koichiro Hori1, Shunsuke Matsuno1, Mayu Sakuma1, Mikio Kishi1, Hiroto Kano1, Yuji Oikawa1, Junji Yajima1
The Cardiovascular Institute, Japan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 61-year-old male presented with a chief complaint of CCS class2 angina. His comorbidities were hypertension, dyslipidemia and end stage renal disease on hemodialysis. He is current smoker. A coronary CT scan conducted six years before had already revealed notable calcification in the left anterior descending artery. Therefore, invasive coronary angiography was planned.

Relevant Test Results Prior to Catheterization
His 12-lead electrocardiogram revealed a state of normal sinus rhythm, devoid of Q waves and any deviations in the ST segment and T waves. Echocardiography showed normal left ventricular function and no regional wall motion abnormalities.
Relevant Catheterization Findings
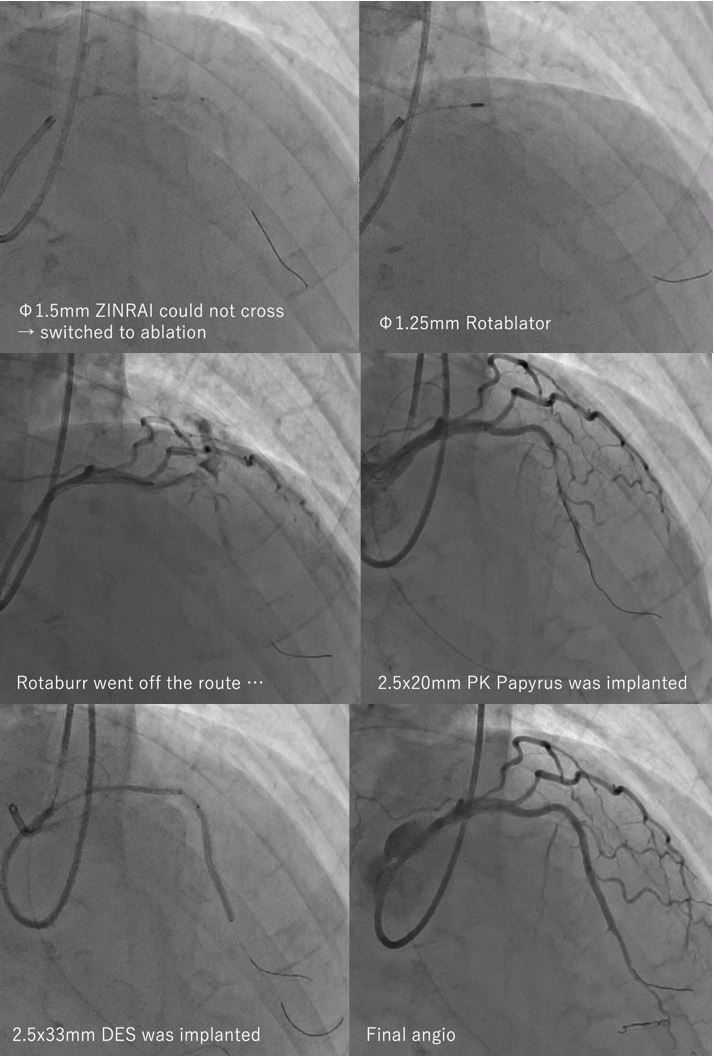
Coronary angiogram revealed a diffuse, heavily calcified stenosis in the bending portion of the mid-LAD.

Interventional Management
Procedural Step
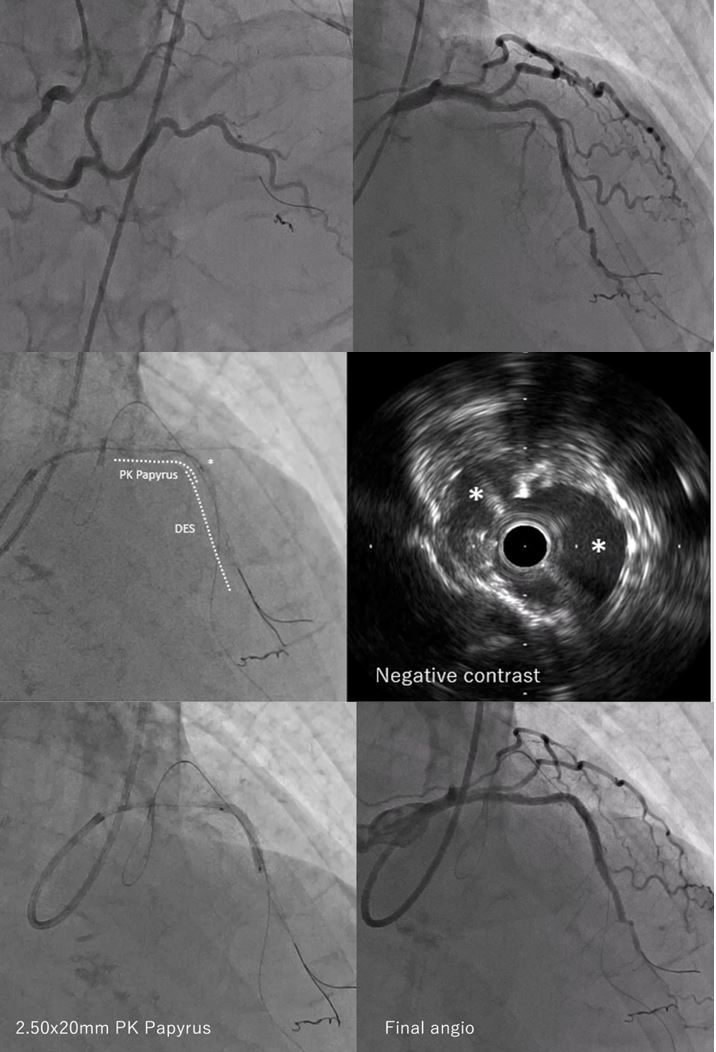
The Guidewire was easily crossed, however IVUS and small balloons could not pass the lesion, so that rotablation was needed. In the 6th ablation, 1.25mm rota burr went off the vessel route and Ellis type 3 coronary perforation was confirmed. His blood pressure soon went down and could not be maintained even with balloon dilatation at the perforation site. Tracheal Intubation and VA ECMO were initiated and pericardiocentesis was performed. Another guiding catheter was engaged for LCA, and covered stent was implanted with angiographical success. ECMO was able to be withdrawn next day and he was extubated on 4POD. On 30POD, the patient had chest pain during rehabilitation with newly appearing pericardial effusion, and was taken to cathlab to check angiogram. We could not confirm extravasation from the angiogram, however, could confirm that the distal egde of the covered stent did not fully attach to the vessel wall because of protruded calcification on the IVUS findings. We assumed that this could cause transient extravasation during rehabilitation and added another covered stent distal to the previous one. After the procedure, pericardial effusion did not appear again, and he was discharged ambulatory without aftereffect.
Case Summary
Coronary perforation caused by rotablator was managed with stent graft implantation. However, a recurrent pericardial effusion, stemming from an endoleak in the sub-acute phase, was noted. The endoleak, attributed to the malapposition of the distal edge of the covered stent owing to protruding calcification, was identified as the causative factor for the recurrent cardiac tamponade. Hemostasis was successfully attained through the additional covered stent implantation for the malapposition site.