
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-140
The Worst Is Yet to Come
By Yushan Chien, Jiunncherng Lin
Presenter
Yu Shan Chien
Authors
Yushan Chien1, Jiunncherng Lin1
Affiliation
Taichung Veterans General Hospital, Taiwan1,
View Study Report
TCTAP C-140
Coronary - Complication Management
The Worst Is Yet to Come
Yushan Chien1, Jiunncherng Lin1
Taichung Veterans General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
This 80-year-old manhas a history of hypercholesterolemia. He felt intermittent lower jaw sorenessduring exercise for 2 years. The discomfort relieved at rest, and he did notpay much attention to it initially. However, the symptoms progressed since about1 month ago that accompanied by cold sweating with merely light physicalactivity. He then came to our cardiology clinic.
Relevant Test Results Prior to Catheterization
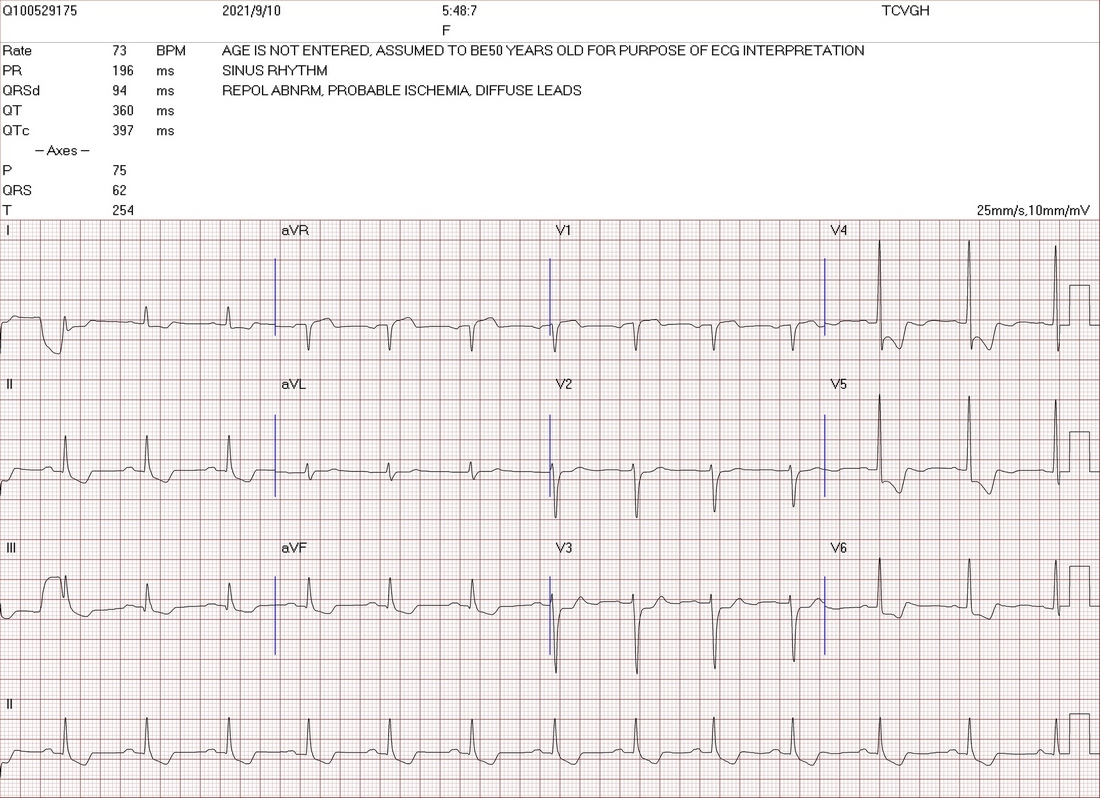
TheECG showed diffuse ST depression.
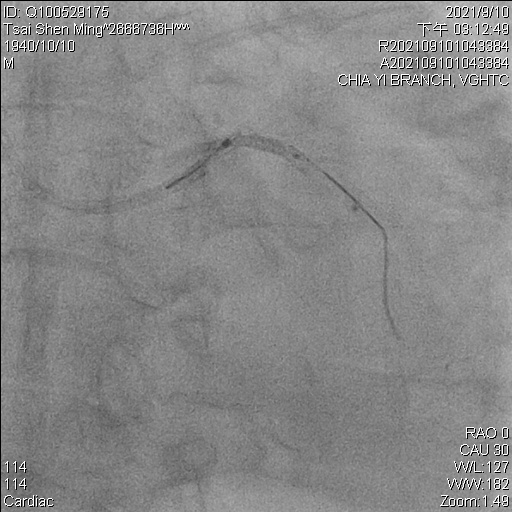
Relevant Catheterization Findings
Theresult of coronary angiography revealed the patient had triple vessel diseasewith left anterior descending artery (LAD) and right coronary artery (RCA)totally occluded and left circumflex artery (LCx) also diffusely diseased. Bypasssurgery was suggested but he refused. Percutaneous coronary intervention was thenproceeded.



Interventional Management
Procedural Step
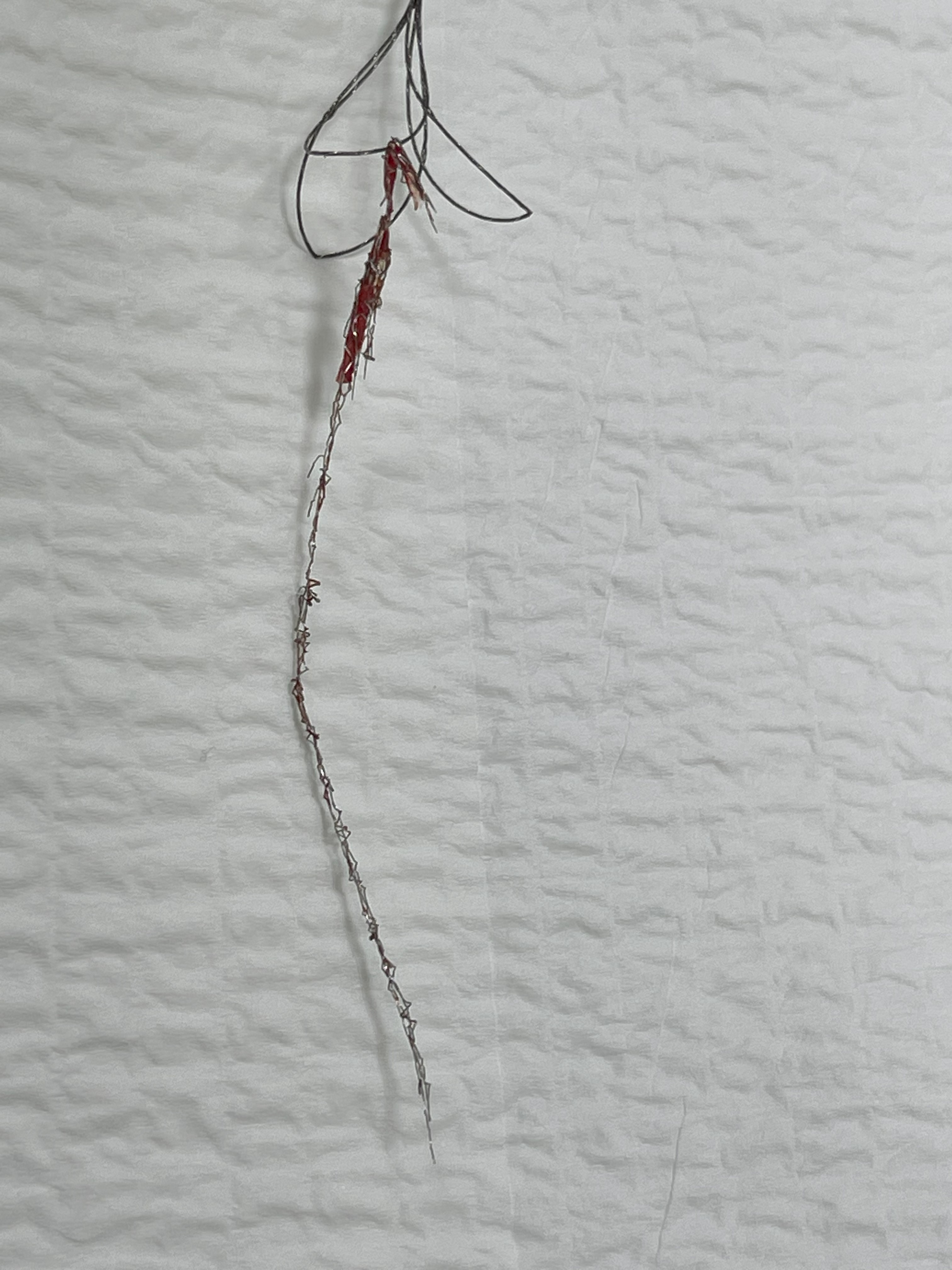
Wetreated RCA and LAD CTO lesions with drug-eluting stents. For the LCx lesion, aSion wire was advanced to the distal and the lesion was pre-dilated. Afterstenting distal LCx with a 2.5x22mm stent, a 3.5x38mm stent was intended to be placedat proximal LCX to OM branch but was dislodged over LM to LCX. We tried to retrievethe stent by small-balloon inflation technique, but the shaft of the balloon fracturedwhen pulling back. We finally caught the broken balloon with a 3.2F Snare andretrieved it. We then tried snaring the dislodged stent, but themicrocatheter of the snare broke when pulling. Fortunately, we took out thebroken microcatheter with a balloon anchored in GC. While withdrawal the microcatheter,the stent was elongated and dragged to the aorta. We changed to a 7 Fr systemand removed the deformed stent with a 6Fr Snare. However, LAD stent wasdeformed and was fixed with another stent after LCx stenting. Though we thoughtall the fragments of metal were removed but indeed some residual stent was protrudedfrom LM to aorta confirmed by CT the next day. Another procedure for LMstenting to crush the residue was performed days later.

Case Summary
The patient wasdoing well and followed regularly at clinic after the procedure. Coronaryangiography was followed 1 year later, and the stents were well without significantin-stent restenosis. There were manyways to manage the complication. When the challenges come one by one, we needto remind ourselves to keep calm to avoid further damage.