
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-104
To Knot or Not to Knot
By Dhiman Banik, Smita Kanungo
Presenter
Smita Kanungo
Authors
Dhiman Banik1, Smita Kanungo1
Affiliation
National Heart Foundation Hospital & Research Institute, Bangladesh1,
View Study Report
TCTAP C-104
Coronary - Complication Management
To Knot or Not to Knot
Dhiman Banik1, Smita Kanungo1
National Heart Foundation Hospital & Research Institute, Bangladesh1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
★60 years Lady.
★Chronic Coronary Syndrome-III (Having exertional chest pain despite optimum medical management).
★Physical examination:-
General Examination-
Pulse: 74 bpm, BP-130/90 mm-Hg with no other significant abnormality.
Systemic Examination: Unremarkable.
★Chronic Coronary Syndrome-III (Having exertional chest pain despite optimum medical management).
★Risk Factor – HTN.
General Examination-
Pulse: 74 bpm, BP-130/90 mm-Hg with no other significant abnormality.
Systemic Examination: Unremarkable.
Relevant Test Results Prior to Catheterization
★Normal blood biochemical parameters.
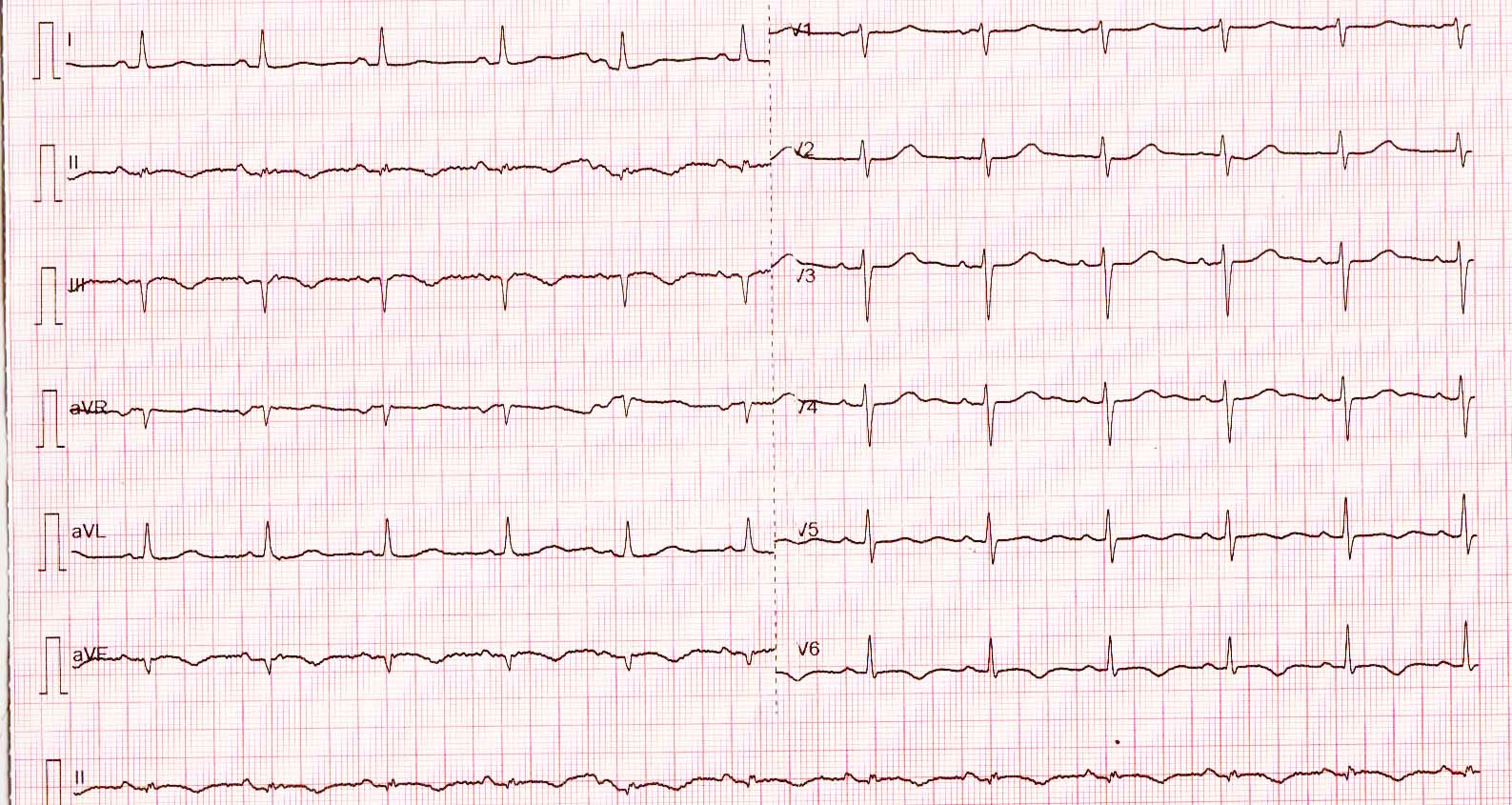
★ECG- T inversion in leads II, III & aVF.
★ECHO: Regional Wall Motion Abnormality (RWMA) with LVEF-40%.
★ECG- T inversion in leads II, III & aVF.
★ECHO: Regional Wall Motion Abnormality (RWMA) with LVEF-40%.
Relevant Catheterization Findings

Interventional Management
Procedural Step
★First, after engaging with the guide catheter, RCA was wired with a run through floppy wire and the lesion was pre-dilated with a 2.0x12mm NC Balloon catheter.
★At first, stent retrieval was attempted with a snare but did not work out as it was small in size.
★Then the next strategy was twirling of wires- two other wires were taken and both the wires were twirled around the dislodged stent. We were trying to make a knot with the double wires over the proximal part of the dislodged stent but unfortunately failed to hold stent.
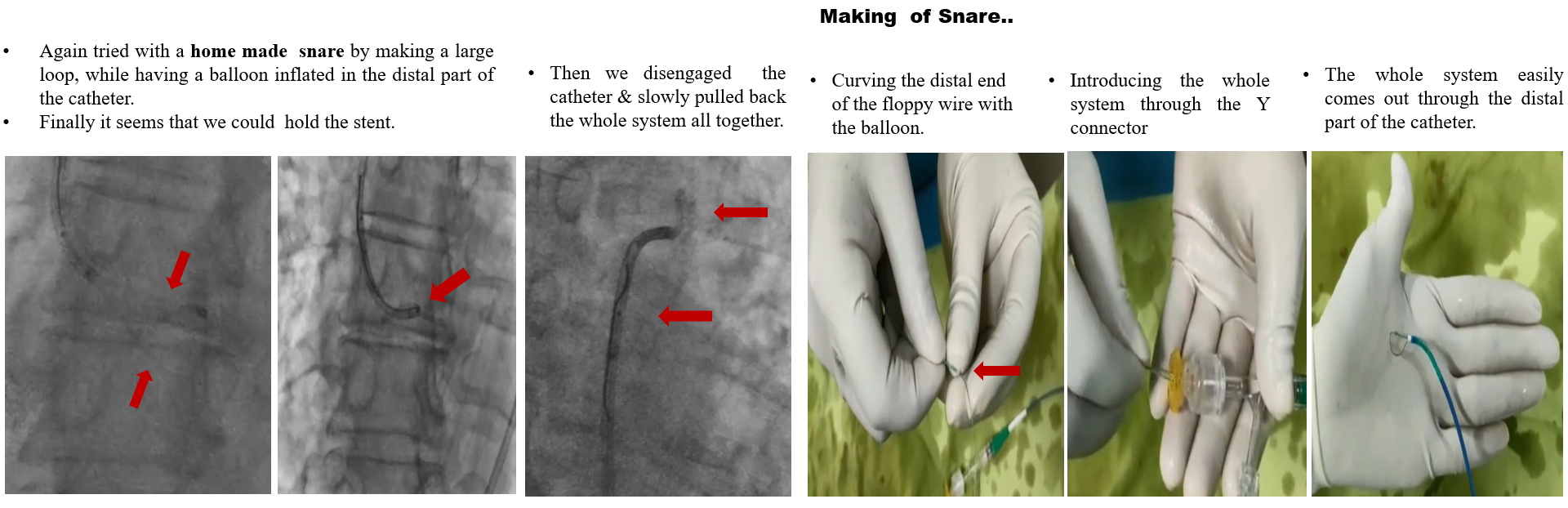
★Then we proceeded with a homemade snare approach. In this method, a large loop was made with floppy wire while keeping a small sized balloon partially inflated at the distal part of the catheter. At this point we succeeded to hold the dislodged stent and brought it back along with the guide catheter.
★Then a new 3.0x 38mm DES was deployed in the RCA with furthermore pre-dilatation and post dilatation.
★A 2.5x40 mm DES was also deployed in LCX and TIMI III flow established.
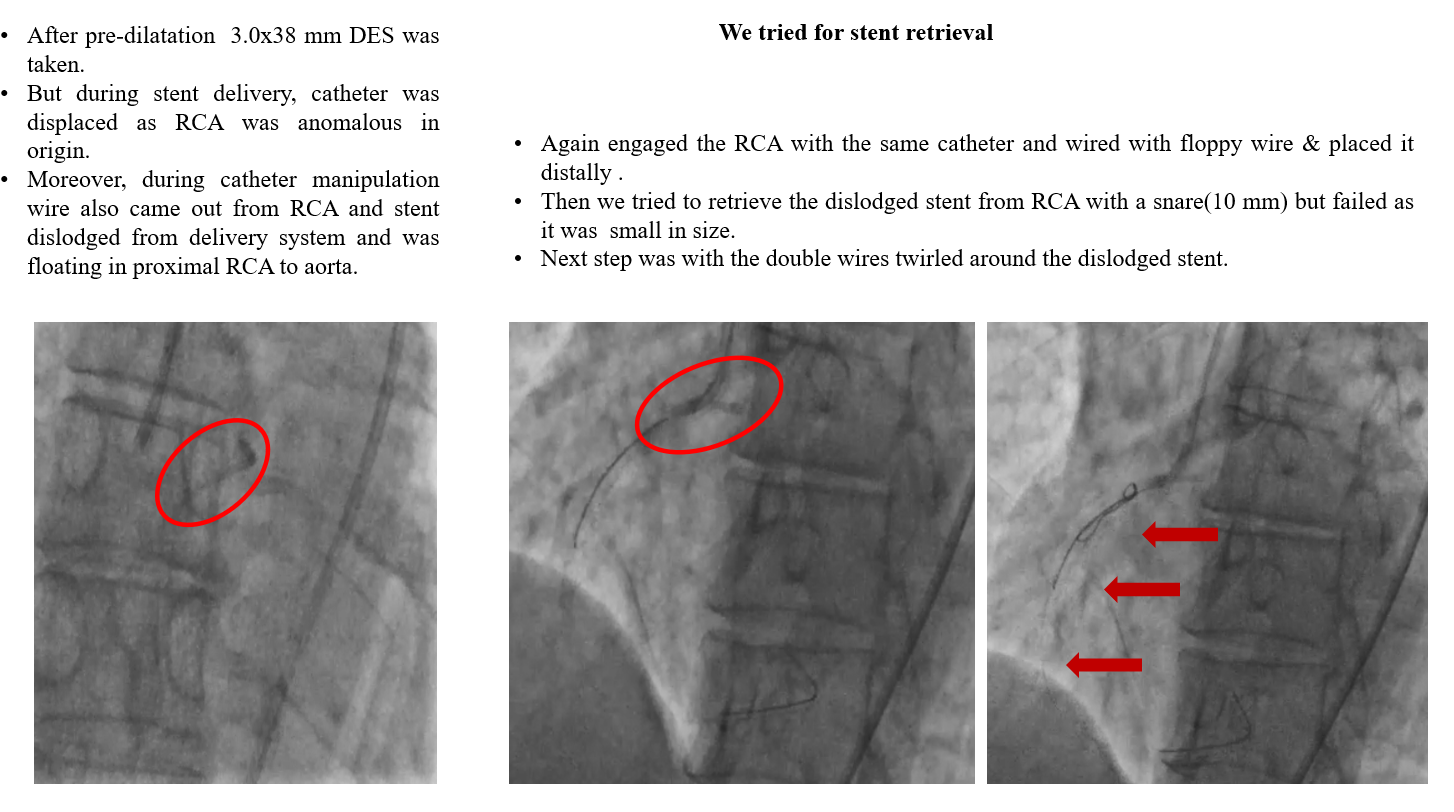

★Then a 3.0x38mm DES was taken to be deployed, but during the stent delivery, the catheter was displaced as RCA was anomalous in origin. Moreover, during catheter manipulation the floppy wire also came out from the RCA and the stent was dislodged from the delivery system, floating in between the proximal RCA and the Aorta.
★After that, stent retrieval strategy was taken. RCA was cannulated once again and wiring was done with a floppy wire which was placed distally. ★At first, stent retrieval was attempted with a snare but did not work out as it was small in size.
★Then the next strategy was twirling of wires- two other wires were taken and both the wires were twirled around the dislodged stent. We were trying to make a knot with the double wires over the proximal part of the dislodged stent but unfortunately failed to hold stent.
★Then we proceeded with a homemade snare approach. In this method, a large loop was made with floppy wire while keeping a small sized balloon partially inflated at the distal part of the catheter. At this point we succeeded to hold the dislodged stent and brought it back along with the guide catheter.
★Then a new 3.0x 38mm DES was deployed in the RCA with furthermore pre-dilatation and post dilatation.
★A 2.5x40 mm DES was also deployed in LCX and TIMI III flow established.
Case Summary
Stent dislodgement can be effectively managed by percutaneous stent retrieval methods. Besides the conventional methods, sometimes innovative measures are needed to be taken, like we succeeded with the help of a homemade snare loop. However, every catheterization laboratory needs to be equipped with instruments for any complexity and familiarizing with these retrieval methods and techniques could be crucial for the interventional cardiologists.