
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-214
Acute Left Ventricle Afterload Mismatch After Percutaneous Mitral Repair
By Sunanto Ng, Amiliana M. Soesanto, Teguh Santoso
Presenter
Sunanto Ng
Authors
Sunanto Ng1, Amiliana M. Soesanto2, Teguh Santoso3
Affiliation
Universitas Pelita Harapan, Indonesia1, Harapan Kita National Cardiovascular Center, Indonesia2, Medistra Hospital, Indonesia3,
View Study Report
TCTAP C-214
Structural - Mitral Valve Intervention - TEER
Acute Left Ventricle Afterload Mismatch After Percutaneous Mitral Repair
Sunanto Ng1, Amiliana M. Soesanto2, Teguh Santoso3
Universitas Pelita Harapan, Indonesia1, Harapan Kita National Cardiovascular Center, Indonesia2, Medistra Hospital, Indonesia3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
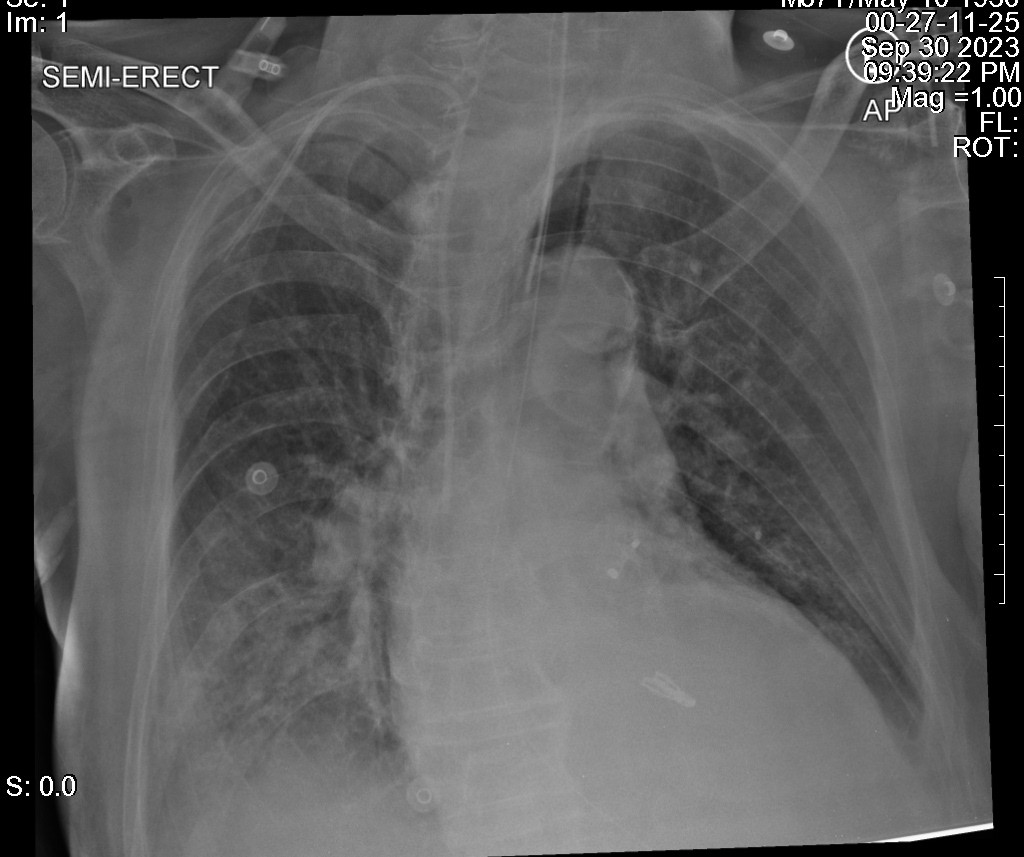
A male patient, 87 year-old, presented with chronic heart failure with reduced ejection fraction. He had a history of percutaneous coronary intervention, atrial fibrillation and implantation of left atrial appendage occluder, chronic kidney disease and chronic limb ischemia. He was treated with optimal medical therapy for heart failure; but, nevertheless, he still experienced impaired exercise tolerance. Blood pressure and heart rate was well controlled at 100/60 mmHg and 60-80 bpm.

Relevant Test Results Prior to Catheterization
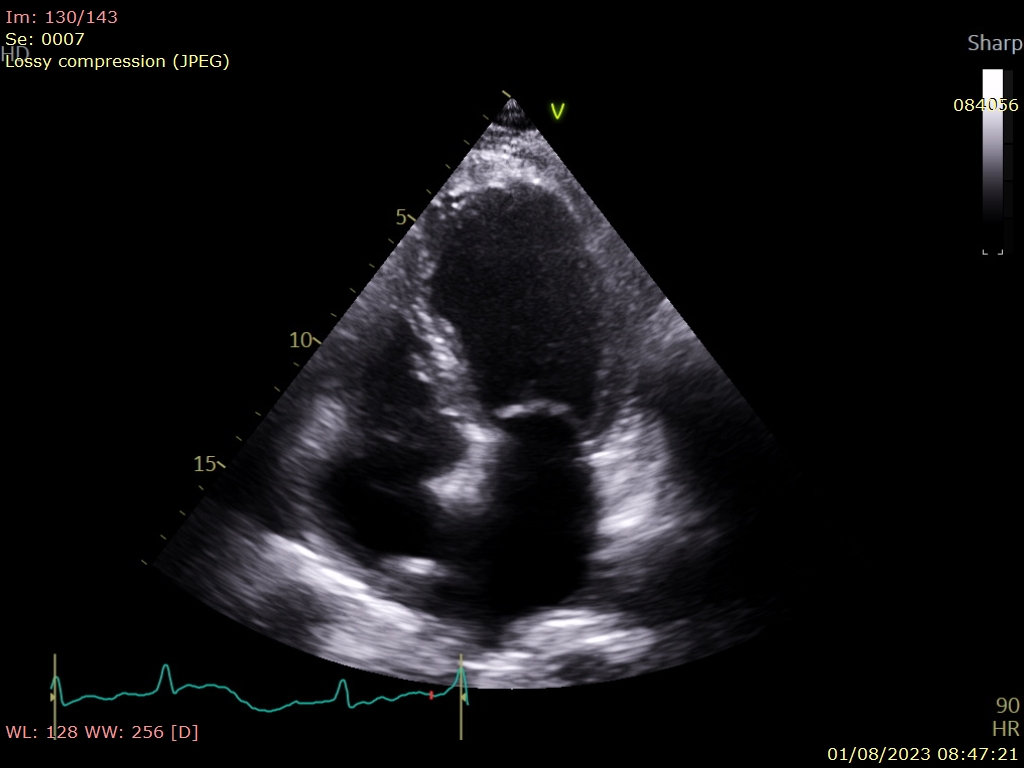
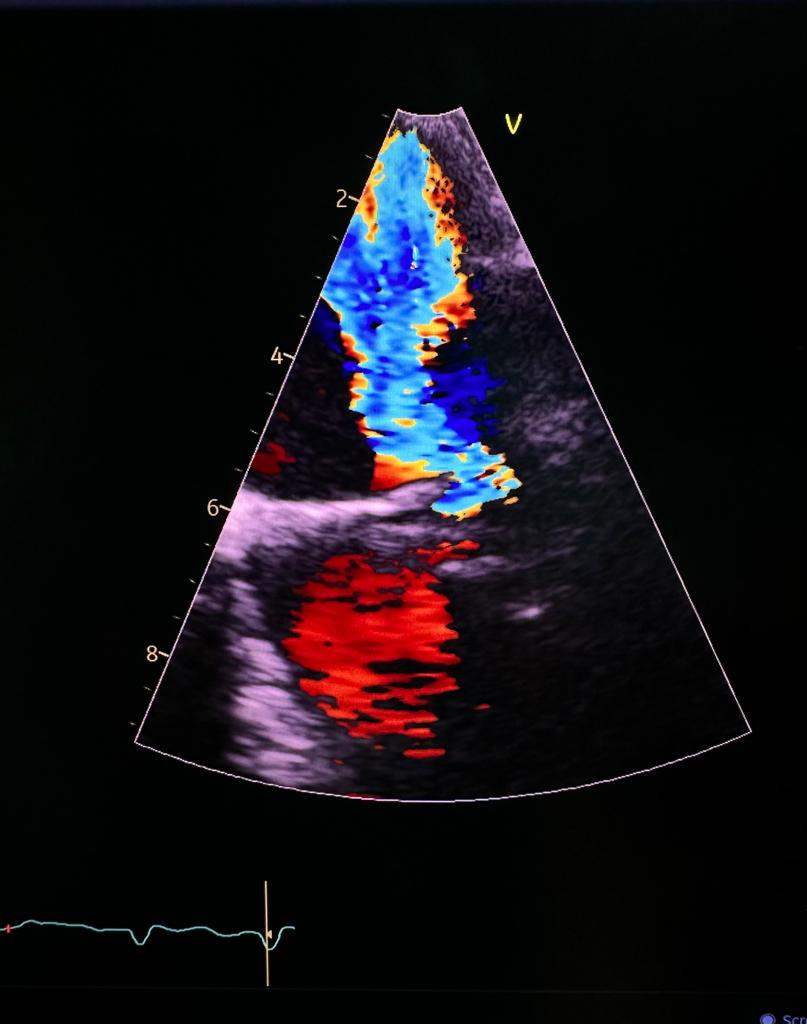
The echocardiogram revealed a dilated left ventricle (LV) with end-systolic diameter of 60 mm (end-diastolic diameter of 70 mm) and dilated left atrium (LA) of 64 mm. The LV end-systolic volume of 111 mL. The LV systolic function was severely reduced (LV ejection fraction 23%), with akinetic LV apex and hypokinetic inferior wall. There was a severe mitral regurgitation (MR) due to annular dilatation and tethering of posterior leaflet. Other valves were normal.

Relevant Catheterization Findings
Interventional Management
Procedural Step
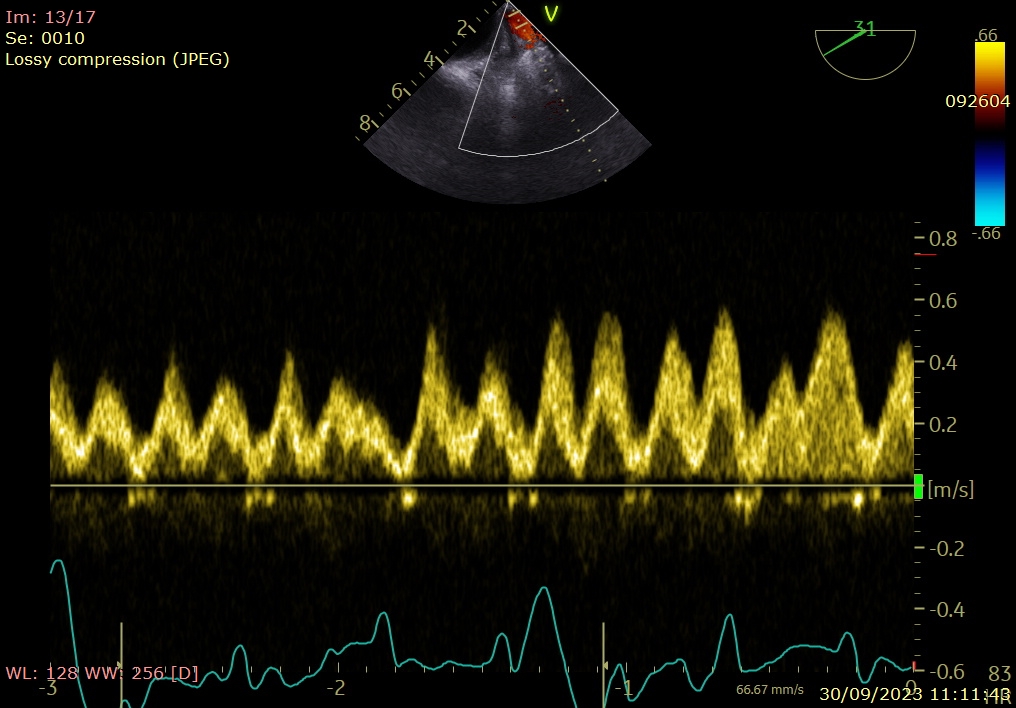
Transcutaneous edge-to-edge mitral repair was done with placement of one MitraClip (Abbott) XTW at A2-P2 scallops. This resulted in trivial MR and disappearance of pulmonary vein systolic reversal with acceptable trans-mitral gradient of 3.5 mmHg.

Case Summary
Percutaneous mitral repair in patients with very poor function is a less invasive and potentially safer alternative to open surgery, but acute LV afterload mismatch may occur. This requires prompt diagnosis and management for a successful outcome.