
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-189
A Difficult Strategy of Double Trouble: Acute Limb Ischemia and Asymptomatic Severe Iliac Occlusion in a Single Limb
By Nathania Purnomo, Isabella Lalenoh, Emanoel Oepangat
Presenter
Nathania Purnomo
Authors
Nathania Purnomo1, Isabella Lalenoh1, Emanoel Oepangat2
Affiliation
Siloam Hospital TB Simatupang, Indonesia1, Siloam Hospital Lippo Karawaci, Indonesia2,
View Study Report
TCTAP C-189
Endovascular - Iliac / SFA Intervention
A Difficult Strategy of Double Trouble: Acute Limb Ischemia and Asymptomatic Severe Iliac Occlusion in a Single Limb
Nathania Purnomo1, Isabella Lalenoh1, Emanoel Oepangat2
Siloam Hospital TB Simatupang, Indonesia1, Siloam Hospital Lippo Karawaci, Indonesia2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 67 years old male came to the ED with acute left calf pain for the past 3 days, with tingling, cold sensation, and worsening claudication. He has a history of hypertension but not regularly taking the medicine, smokes 2 packs of cigarettes per day, and no history of cardiovascular event. Upon admission, his blood pressure was 150/80 mmHg, his left calf revealed pallor, paresthesia, and poikilothermy. Arterial pulses below left common femoral artery were not palpable.
Relevant Test Results Prior to Catheterization
ECG showed sinus rhythm and left atrium enlargement.
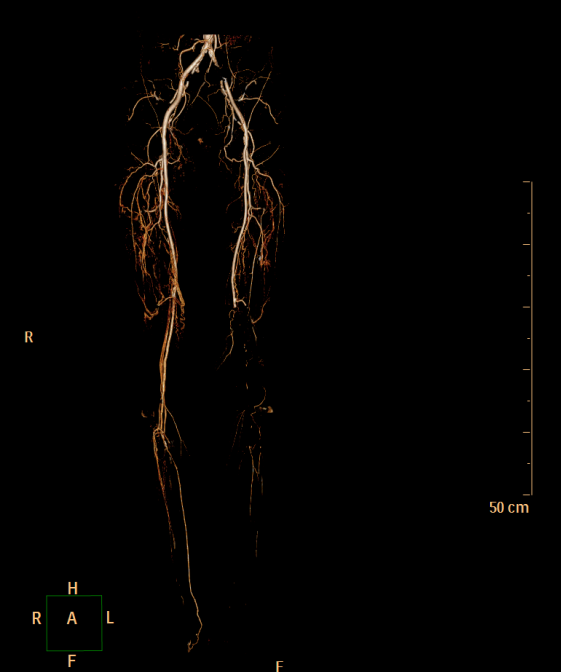
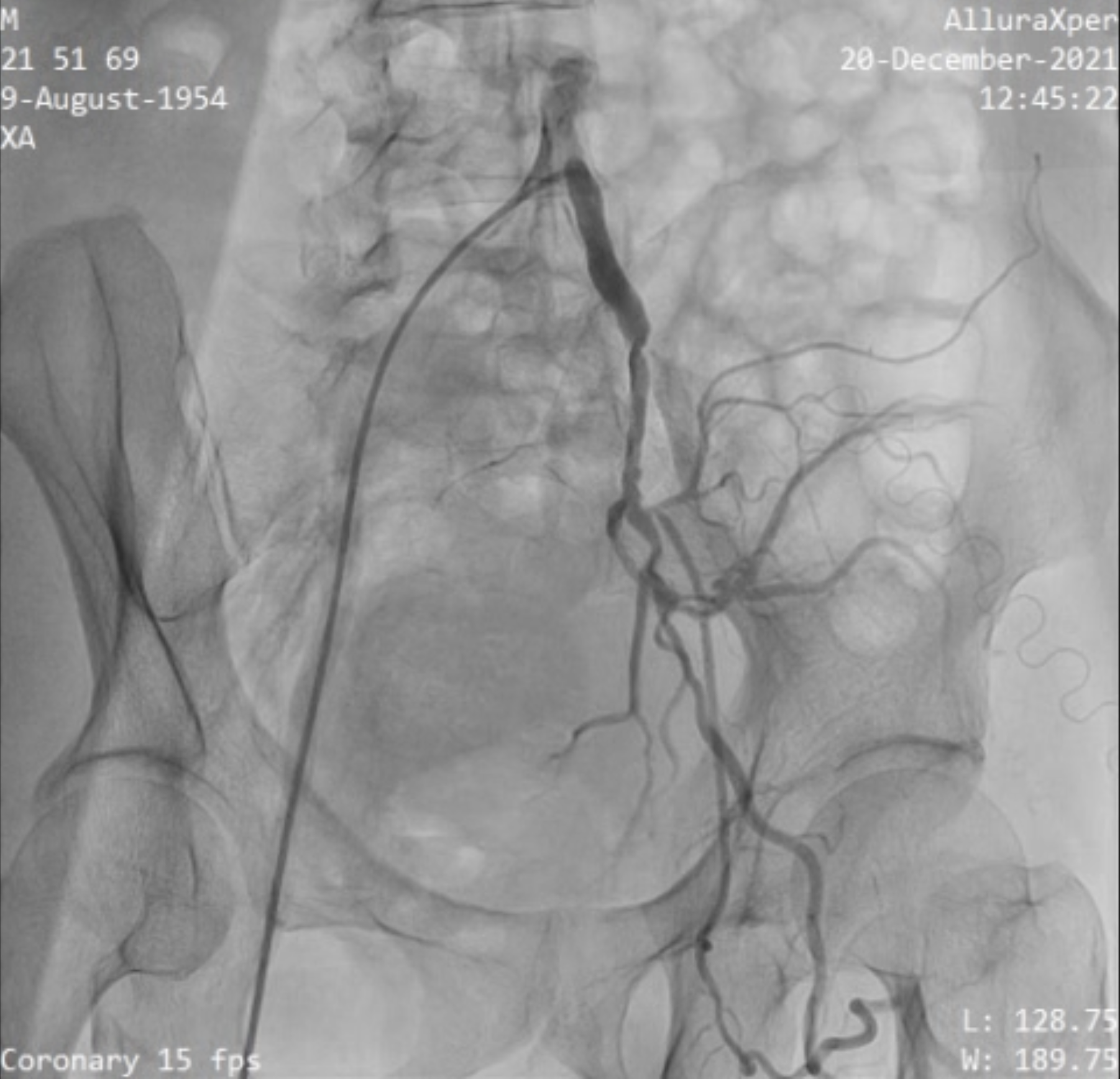
Relevant Catheterization Findings
- Complete total occlusion and severe stenosis of left common iliac artery- Complete total occlusion of distal SFA as the cause of acute limb ischemia event


Interventional Management
Procedural Step
A 6 Fr sized femoral sheath was inserted into the right common femoral artery, and JR 4/6 F was used to access the iliac bifurcation for a cross-over approach. A total occlusion of the ostial external iliac artery was found at the level of the iliac artery bifurcation, with reconstitution at the distal part through the internal iliac artery collaterals. The 0.35 GW wire could not pass through the occlusion. Therefore, we used a V-18 wire to navigate through the CTO with difficulty and finally placed it intraluminally. Predilation was done with a Mustang 6.0/60mm balloon, establishing blood flow to the distal SFA and the internal iliac artery. Then, thrombotic occlusion at the distal SFA was identified as the cause of the ALI event. Complete total occlusion at the distal SFA was passed through with V-14 wire. Due to heavy thrombus burden, mechanical thrombus aspiration was performed from the distal SFA to the mid-distal posterior tibial artery using the Angiojet® System Solent Dista 145/4F. After several runs, significant stenosis was revealed along its length. Balloon angioplasty, using a Coyote 3.0/220mm/150 balloon, was then carried out from the distal SFA to the distal posterior tibial artery. The occluded anterior tibial artery was then rewired using V14 CW, followed by another round of balloon angioplasty with the Coyote 3.0/220/150 balloon. Angiographic evaluation confirmed the successful restoration of blood flow from the common iliac artery to the arch of the pedis.



Case Summary
The clinical features of ALI at distal SFA were very evident in this case. Unexpectedly, a concurrent discovery was made during CT angiography, revealing an asymptomatic severe occlusion of the left common iliac artery. This finding added complexity to the revascularization process with wire manipulation to traverse the occluded common iliac artery and finally reach the source of the ALI. Mechanical thrombus aspiration, whether standalone or in combination with other modalities like angioplasty, proves to be a safe and effective management strategy for ALI. The goal is to improve rates of limb salvation and reduce the need for open surgical embolectomy or catheter-directed thrombolysis.