
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-095
A Rare Case Report: Floating Wire Technique in Isolated Ostial Left Main Coronary Artery Disease
By Adriyawan Widya Nugraha, Arief Wibisono, Evit Ruspiono, Tri Astiawati, Fitranti Suciati Laitupa
Presenter
Adriyawan Widya Nugraha
Authors
Adriyawan Widya Nugraha1, Arief Wibisono1, Evit Ruspiono1, Tri Astiawati1, Fitranti Suciati Laitupa1
Affiliation
Dr. Iskak Tulungagung Hospital, Indonesia1,
View Study Report
TCTAP C-095
Coronary - Complex PCI - Left main
A Rare Case Report: Floating Wire Technique in Isolated Ostial Left Main Coronary Artery Disease
Adriyawan Widya Nugraha1, Arief Wibisono1, Evit Ruspiono1, Tri Astiawati1, Fitranti Suciati Laitupa1
Dr. Iskak Tulungagung Hospital, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
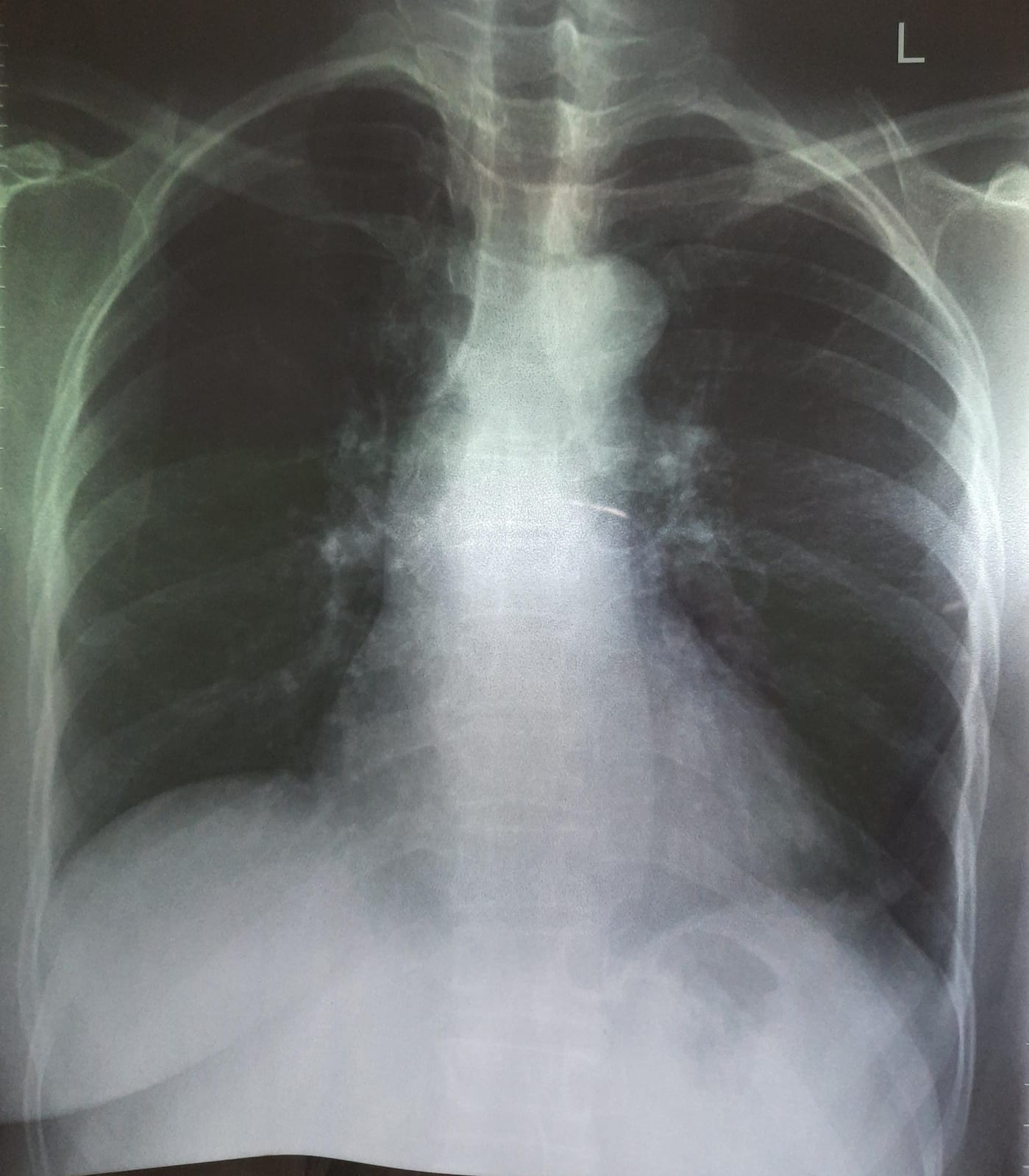
A 50-year-old woman presented angina pectoris CCS II and mild shortness of breath during moderate activity. She felt symptoms worsening since 7 months ago. Six months ago patient came to another hospital with acute coronary syndrome. The risk factor smoker, diabetes mellitus hypertension, and dyslipidemia were denied. Based on clinical physical examination the vital sign was normal. We only found systolic murmur at the apex others were within normal limits.
Relevant Test Results Prior to Catheterization
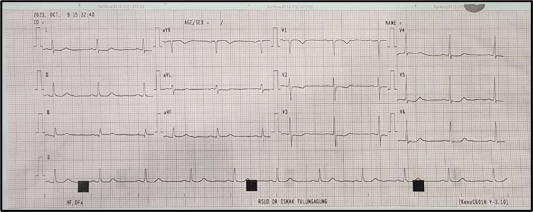
Patient has typical chest pain and shortness of breath during activity with a previous history of ccute coronary syndrome. The ECG showed ST depression in lead V1-V6 and T inversion in lead V1 and V2. Based on the echocardiography results supported regional wall motion abnormalities, so we decided to do adhoc coronary angiography and percutaneous coronary intervention if significant stenosis was found.
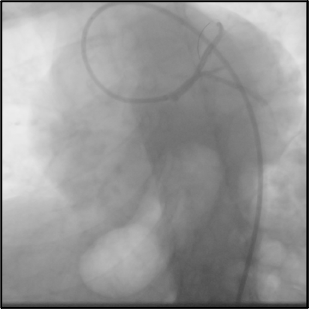
Relevant Catheterization Findings
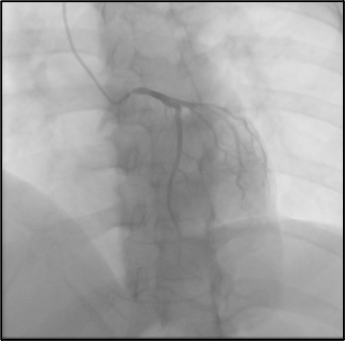
Angiography was performed via radial access with a 6Fr sheath and TIG 5Fr catheter for Coronary Angiography (CAG) and heparin 6500 International Unit (IU) intra-vein was injected. Based on CAG was shown right dominance coronary artery and stenosis ostial LM 70-80%, other coronary was within normal and there was no significant stenosis. Following the procedure CAG the hemodynamic pressure was always decreased because of catheter damping when the catheter diagnostic engaged into ostial LMCA.
Interventional Management
Procedural Step
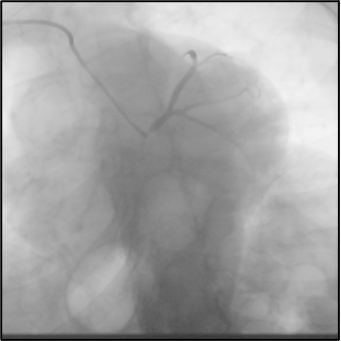
Considering LM disease and we will evaluate LM using Intravascular Ultrasound (IVUS) and the risk of hemodynamic disturbance, we decided to continue coronary intervention by switching access via femoral access by using the EBU 7.5F approach with a side hole for guiding catheter for coronary intervention. We used workhorse wire Runtrough NS Hypercoat for crossing LM to the left anterior descending coronary artery (LAD). Pre-dilated with balloon semi-compliance 2.5 x 10 mm in ostial LM. After pre-dilatation with a semi-compliance balloon, IVUS was performed to assess the diameter of LM disease. To prevent failure of stent placement and ensure proper stent placement without hemodynamic disturbances due to catheter damping which causes a decrease in arterial pressure to the coronary arteries, we decided to use a floating wire technique using workhorse wire Hypercoat NS Runtrough. Stent DES 4.0 x 12 mm was implanted in ostial-mid LM inflated to 14 atmospheres. After that, we used balloon non-compliance (NC) 4.0 x 12 mm inflated to 18 atmospheres for the post-dilatation stent. IVUS was again used to evaluate stent implantation. Based on IVUS post PCI we did not find stent edge dissection, MSA was 11,9 mm2 and the diameter of stent was around 4.6 mm. The stent was well apposition and the final result angiography was good TIMI flow was 3. We decided to stop the procedure without finding hemodynamic disturbance, or post PCI complications.
Case Summary
Ostial LM Percutaneous coronary intervention (PCI) is one of the challenges that need a special technique to prevent cardiac complications during the procedure. The floating wire technique is one of the main techniques for facilitating aorta-ostial intervention. We report patient female 50 years old who has typical chest pain and history of ACS. In this case, We decided on a side-hole catheter using EBU 7Fr of guiding catheter and the floating wire technique approach for stenting LM coronary to prevent dampening pressure hemodynamic during PCI due to aorta-ostial lesion. Also we are using IVUS to assess LM coronary profile. The procedure was good without any cardiovascular complications event.