
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-110
It Never Rains but It Pours
By Mohd Khairi Othman, W Yus Haniff W Isa, Zurkurnai Yusof
Presenter
Mohd Khairi Othman
Authors
Mohd Khairi Othman1, W Yus Haniff W Isa1, Zurkurnai Yusof1
Affiliation
Universiti Sains Malaysia Hospital, Malaysia1,
View Study Report
TCTAP C-110
Coronary - Complication Management
It Never Rains but It Pours
Mohd Khairi Othman1, W Yus Haniff W Isa1, Zurkurnai Yusof1
Universiti Sains Malaysia Hospital, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 50-year-old man with underlying type 2 diabetes mellitus, hypertension, and psoriasis presented to our center with a complaint of central chest pain for 3 days, worsening on the day of admission. The left-sided chest pain was characterized as crushing in nature, with a pain score of 8/10. Upon examination, BP was 110/90mmHg, and PR was 100bpm. Other clinical examination unremarkable.

Relevant Test Results Prior to Catheterization
Initial electrocardiography showed sinus rhythm with ST elevation at V2-V4. A diagnosis of anterior myocardial infarction was made, and thrombolysis with intravenous tecnetaplase was given. Echocardiography showed hypokinesia at the anteroseptal, septal, and anterior LV wall hypokinesia. Subsequently, he underwent a pharmacoinvasive PCI to LAD with a planned staged PCI to LCx.
Relevant Catheterization Findings
LMS: NormalLAD: Proximal irregular 20% then 99% at midLAD.LCx: Tortous proximal, small distal. Proximal OM functional CTO and received collaterals from LAD.RCA: Co-dominant. Distal 50%
During index procedure, we performed PCI to midLAD and plan for staged PCI to Lcx-OM.
During index procedure, we performed PCI to midLAD and plan for staged PCI to Lcx-OM.
Interventional Management
Procedural Step
The attempt of PCI to LCx CTO was performed on 26 Oct 2023. Using a CLS 3.0 guiding catheter and Whisper MS, a guidewire was used to cross the LCx CTO. Because of the tortuosity of the LCx, a Guidezillla II is a guide extension for better support. The Corsair Pro microcatheter was also used to support the guidewire to cross the CTO. After a few wiring attempts, the CTO, unfortunately, noted the guidewire tip was broken off. The remnant of the guidewire was floating in the proximal LCx. Decided to attempt to snare the remnant of guidewire. Using a snare of 2mm, however, the attempt to snare failed despite the assistance of a Guidezilla II extension catheter. The remnant of the guidewire moves the LAD from the initial position. A reattempt to use snare at the LAD failed. A predilation balloon Ryurei 1.5x10mm was used as an anchor to snare the guidewire remnant. The predilatation balloon was inflated up to 17 atm but failed to snare the remnant. The strategy of change to using two guidewires and purposely twisting over the guidewire remnant was used. After two twisting attempts, the guidewire remnant could snare out from the LAD. Immediate after the procedure, a contrast injection showed a flow limiting dissection at the previous stent distal edge with TIMI 0. The LAD rewired with new guidewire. A Ryurei 1.5x10mm was used up to 22 atm. A Resolute Onyx 2.75x15mm deployed and overlapped with previous stent.

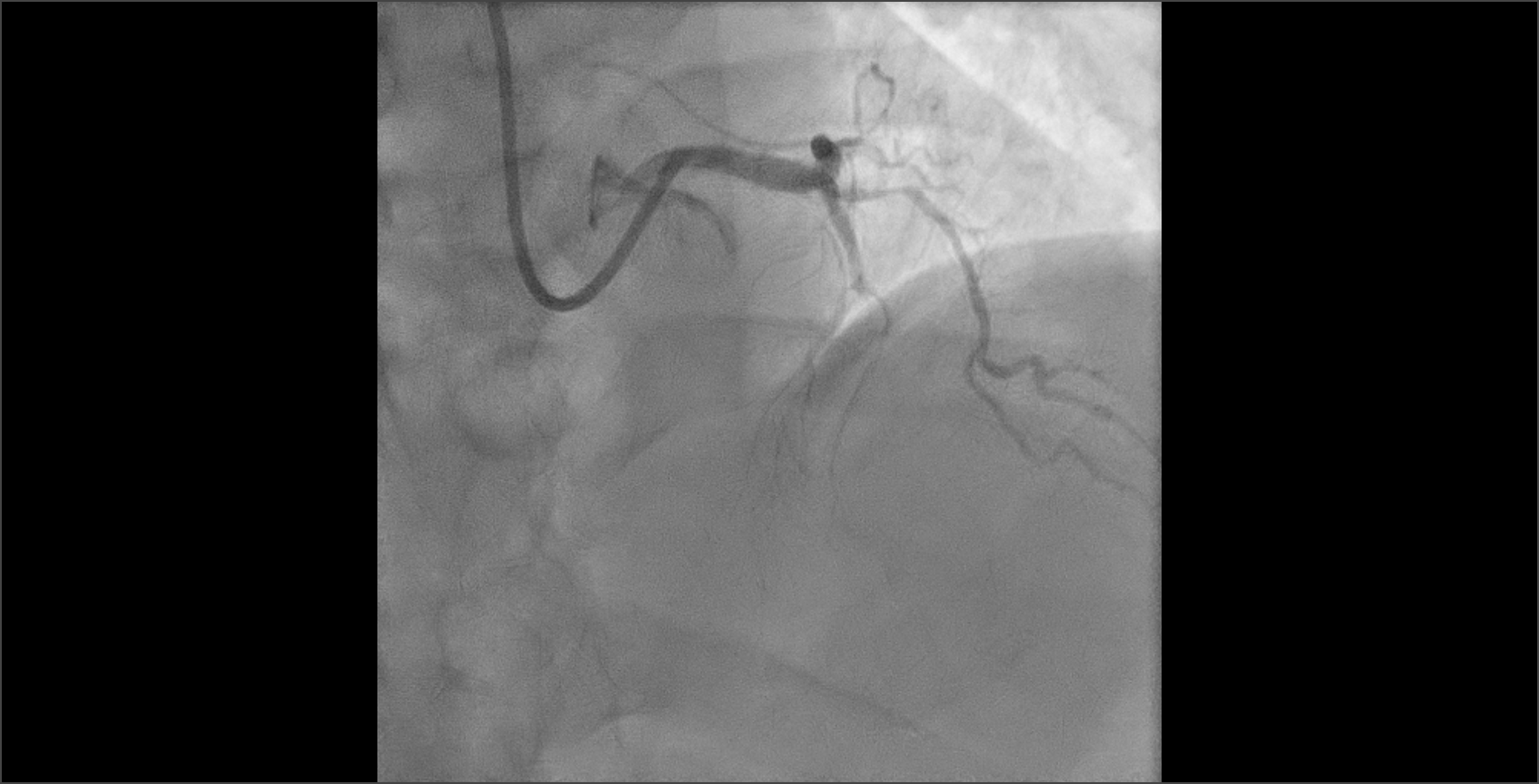
 No flow at the LAD after fracture guidewire removal.png
No flow at the LAD after fracture guidewire removal.png

Case Summary
Guidewire fracture is a rare complication in interventional cardiology. It is important to remind of this complication when manipulating a guidewire with microcathether in very tortuous vessel. Using additional guidewire to remove the fracture segment is one of the method of managing this complication. By using this method, it is mandatory to anticipate risk of coronary artery dissection which shown in this patient.