
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-084
Enhancing Precision in Complex PCI: A Case Report of CTO In-Stent Restenosis Intervention Guided by Optical Coherence Tomography
By Mardlatillah Affani, Muhammad Syukri
Presenter
Mardlatillah Affani
Authors
Mardlatillah Affani1, Muhammad Syukri1
Affiliation
RSUP. Dr. M. Djamil Padang, Indonesia1,
View Study Report
TCTAP C-084
Coronary - Complex PCI - In-Stent Restenosis
Enhancing Precision in Complex PCI: A Case Report of CTO In-Stent Restenosis Intervention Guided by Optical Coherence Tomography
Mardlatillah Affani1, Muhammad Syukri1
RSUP. Dr. M. Djamil Padang, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 71-year-old man presented with CCS III refractory angina despite optimal medical therapy. The patient had a long history of non-adherences medication and follow up. His cardiovascular risk factors were dyslipidemia, ex-smoker, and hypertension. This patient is known as a single-vessel disease(1VD) patient with a series of interventions due to recurrent in-stent-stenosis (ISR). Multiple PCI using the combination of 1 BMS (2007) dan 2 DES(2008), followed by multiple POBA (2009-2020).
Relevant Test Results Prior to Catheterization
The laboratory findings were within normal limit. The electrocardiogram showed sinus rhythm, poor R wave progression with T wave depression of the anterior segments. The echocardiogram revealed reduced left ventricular ejection fraction (34%) with hypokinetic of the anterior wall.

Relevant Catheterization Findings
Coronaryangiography demonstrated a chronic total occlusion (CTO) of the proximal leftanterior descending artery (LAD), classified as ISR type IV.


Interventional Management
Procedural Step
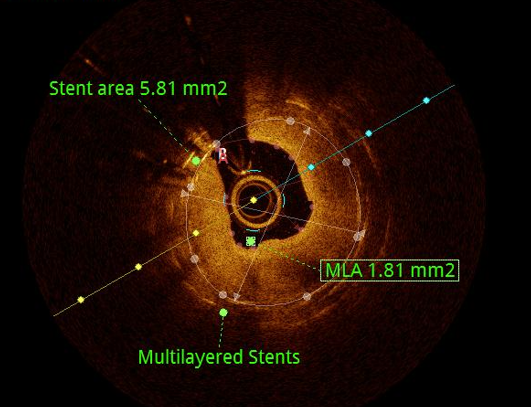
The PCI for CTO ISR was performed using an antegrade approach, successfully crossing the lesion using a Miracle 6 guidewire supported by a microcatheter. We opted for an Optical Coherence Tomography (OCT)-guided. The OCT imaging demonstrated both mechanical and biological problem. It revealed suboptimal expansion in both the distal and multilayered stent part along with the presence of a diffuse neo-atherosclerotic lesion. We used 2.5x15 mm and 3.5x15 mm scoring NC balloon inflated up to 20 ATM for lesion preparation. To overcome the mechanical issues in multilayered area of the stent, we elected to apply high pressure balloon Pro HP 4.0x10 mm up to 24 ATM. The OCT image post-balloon dilatation demonstrates multiple plaque disruption, no medial dissection, good stent expansion, and optimal lumen gain was achieved. Subsequently, a drug-eluting balloon (Paclitaxel) 3.5x20 mm was employed to optimize the result.

Case Summary
The procedure described was the first intracoronary imaging-guided PCI the patient underwent after multiple instances of ISR. This case highlights the importance of meticulous imaging-guided intervention and the potential for achieving favorable outcomes in patients with complex coronary artery disease presentations and the use of drug-coating balloon as the treatment of ISR could be used to prevent multilayered stenting. Prevention of ISR by proper lesion preparation, adequate lesion coverage, and use of intravascular imaging to guide stent placement is preferable.