TCTAP C-032
Coronary - Complex PCI - Calcified Lesion
Against All Odds
Kai Soon Liew1, Vijayendran Rajalingam2, Yuen Hoong Phang1, Kenneth Kay Leong Khoo1, Huan Yean Kang1, Aditya Fahmi Prianda3, Chai Yih Tan1, Kantha Rao Narasamuloo1, Saravanan Krishinan4, Chee Tat Liew5, Dharmaraj Karthikesan6
Sultanah Bahiyah Hospital, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2, Hasna Medika Kuningan Heart Hospital, Indonesia3, Ministry of Health Malaysia, Malaysia4, Pantai Penang Hospital, Malaysia5, Hospital Sultanah Bahiyah, Malaysia6,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 83 year old lady with symptomatic severely calcified triple vessels disease was referred from a private hospital for intervention. Pre-morbidly patient was ADL independent and enjoyed doing her gardening daily. She has now daily chest pain which prevents her from enjoying her daily activities. After a detail heart team discussion, along with patient and her family members, a high risk multi-vessel full re-vascularisation was planned.

Relevant Test Results Prior to Catheterization
ECG showing sinus rhythm, Q wave over the anterior leads
Relevant Catheterization Findings
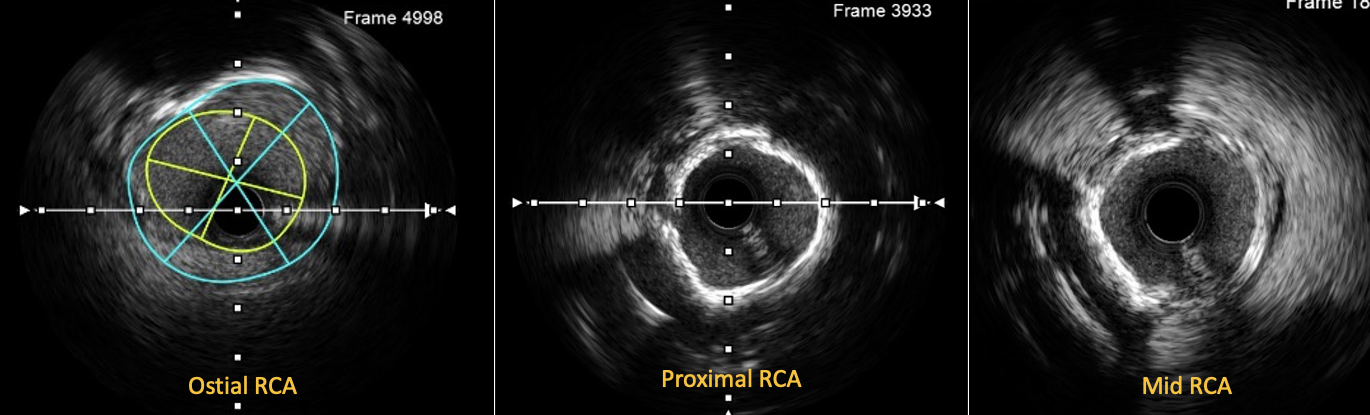
Diagnostic angiogram showed severely calcified triple vessel disease. A chronic total occlusion of the left anterior descending artery, a recessive left circumflex artery and a Shepherd's crook right coronary artery with ostial disease. IVUS confirmed severely calcified vessels as well, evidence of myocardial bridging in distal LAD.

Interventional Management
Procedural Step
Short tip JL3.5 guider engaged and LAD wired with Gaia 1
st in Finecross. Sion blue wired to OM1 for extra support. Failed to advance thus changed to Cosair pro. Guider dislodged while advancing microcatheter. Rewired LAD with Fielder XTR and prepared with 0.8-1.5 balloon sequentially. Exchanged to Runthrough wire and further prepared with 2.0 balloon. IVUS showed 360° calcium. LAD prepared with 2.5 and 3.0 scoring balloon. IVUS showed calcium ring cracked. LM to pLAD stented with 3.5x33 and POT done to LM. IVUS noted stent well expanded. pLAD stented with 2.5x22 and NC with 3.5x15. Patient became hypotensive and ECHO revealed pericardial effusion 2.2cm. Contrast via microcatheter noted dLAD wire perforation. Prolonged inflation with a 1.0 balloon sealed perforation. Final IVUS showed good results and no pericardiocentesis done. Stage PCI to RCA via JR4.0 guider with temporary pacemaker support. Fielder XTR crossed lesion in Finecross to PDA but failed to advance microcatheter. Guidezilla aided Finecross pass mRCA lesion.Unable to send rotablator, found stuck in guider. Able to send up rotablator after prepared in-vitro but guide is not coaxial. Ostial lesion prepared with Wolverine and successfully send down burr. 5 runs done and patient develoepd PEA and CPR for 2 minutes. Lesion predilate with 1.5 and 2.0 balloon then with a 3.0 scoring balloon. IVUS noted circumferential calcium at mRCA- pRCA. IVL done with a 3.5x12 balloon. Two 3.5x38 stent deployed from ostial to mRCA.



Case Summary
In CHIP cases, advance planning is utmost important before embarking on the procedure. In this case, choosing the right stents is crucial due to patient’s high bleeding risk profile. Usage of imaging is mandatory, be it lesion assessment or optimizing stent, but also to reduce contrast usage in the geriatric age group. Hybrid calcium ablation involving rotablation and IVL is occasionally required due to the nature of the lesion. Lastly, understanding of vessel anatomy, as in this case, a Shepherd’s crook right coronary artery, the choice of guiding catheter is important to ensure coaxial fitting and sufficient support and usage of guide extension to navigate past tortuous segments.
