
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-180
Optical Coherence Tomography Guided Management of Calcific Nodule With Intravascular Lithotripsy
By Saurabh Dhumale, Debdatta Bhattacharyya
Presenter
Saurabh Dhumale
Authors
Saurabh Dhumale1, Debdatta Bhattacharyya2
Affiliation
Narayana Health Rabindranath Tagore International Institute of Cardiac Sciences, India1, RN Tagore Hospital, India2,
View Study Report
TCTAP C-180
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
Optical Coherence Tomography Guided Management of Calcific Nodule With Intravascular Lithotripsy
Saurabh Dhumale1, Debdatta Bhattacharyya2
Narayana Health Rabindranath Tagore International Institute of Cardiac Sciences, India1, RN Tagore Hospital, India2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
57 year old hypertensive, non-diabetic gentleman had an episode of sudden severe chest pain a week prior to presenting in the outpatient department. He was treated at an outside hospital where he underwent angiography and was referred to us for revascularisation. On presentation, patient complained of CCS Class III angina and NYHA Class II shortness of breath. On examination, he had stable hemodynamics, cardiovascular examination was insignificant with no signs of heart failure.
Relevant Test Results Prior to Catheterization
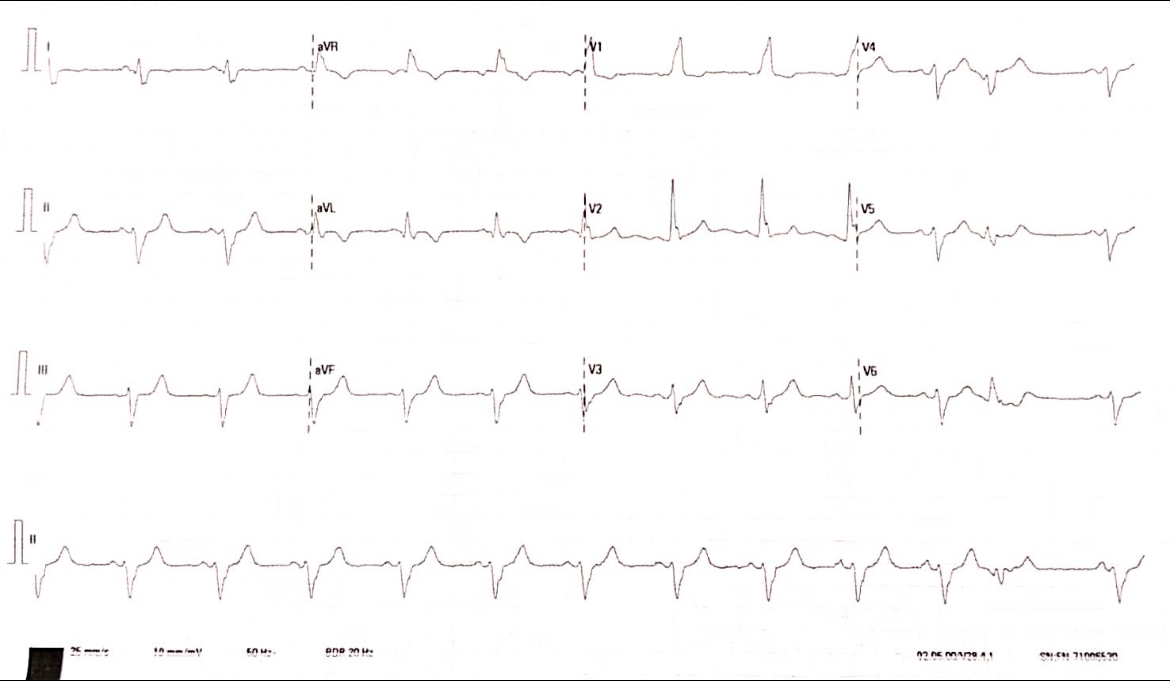
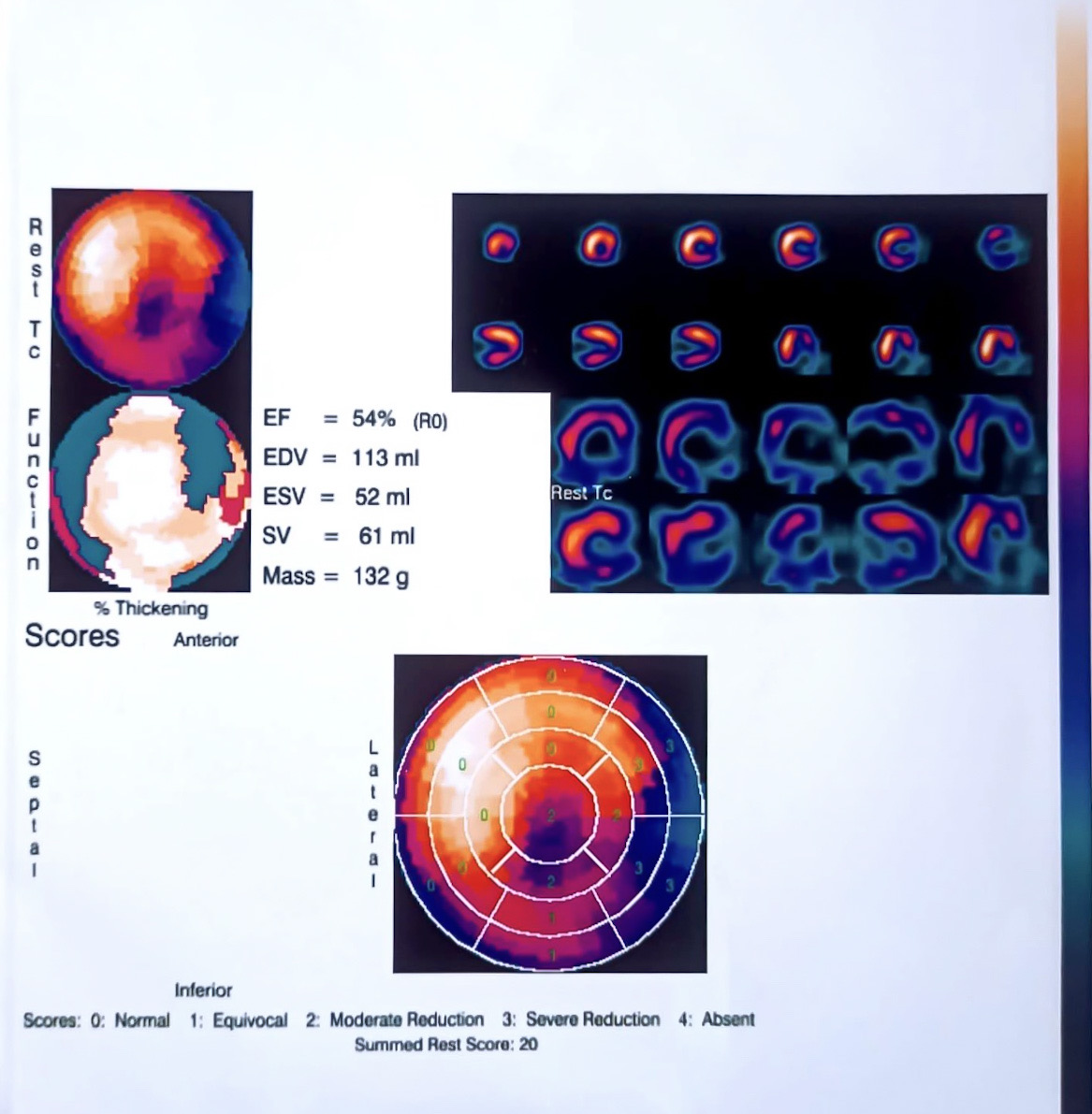
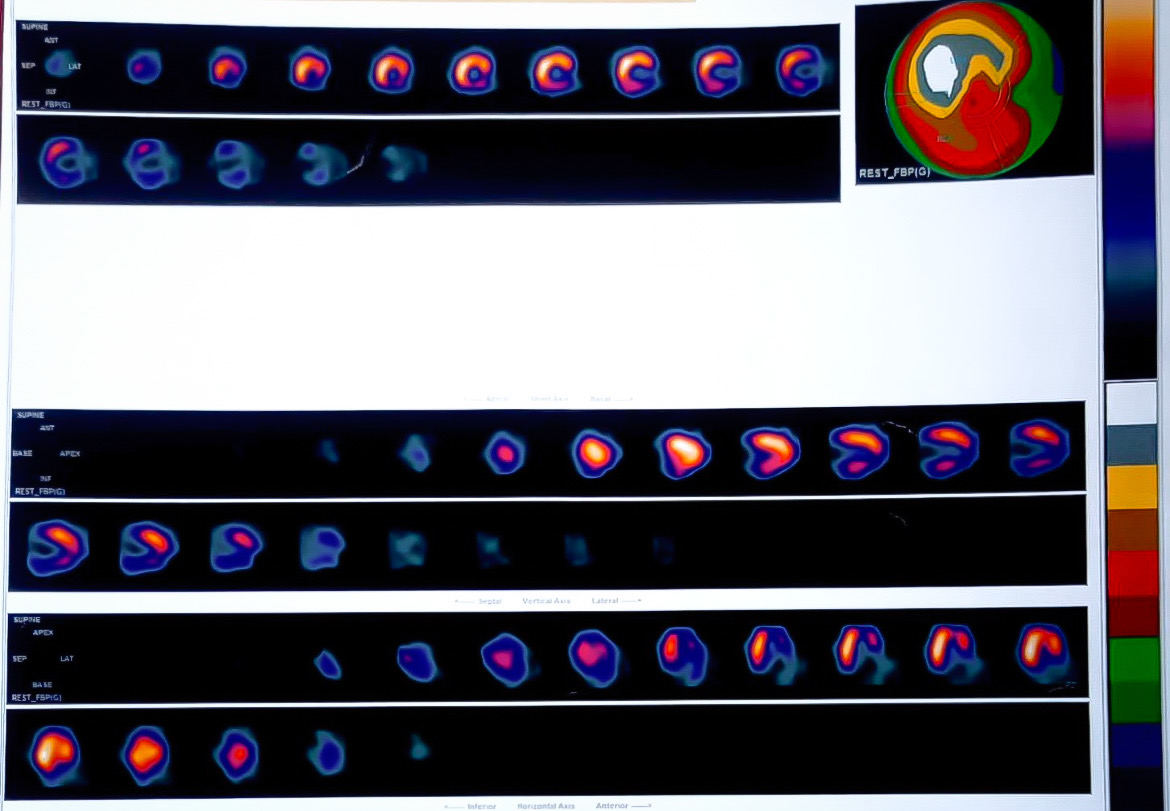
His routine blood work-up did not reveal any significant abnormality, while his hs-Troponin I levels were elevated. ECG revealed bifascicular block with ST depression in anterior precordial leads. ECHO revealed RWMA+ with LV ejection fraction of 45%. A SPECT scan for viability assessment was performed in view of late presentation of the patinet, it revealed infarcted LCX territory with viable rest of the myocardium.
Relevant Catheterization Findings
The angiogram revealed a dominant disease free RCA, LcX CTO without significant retrograde filling and a calcific mid-LAD 85% stenosis with ruptured plaque appearance.
Interventional Management
Procedural Step
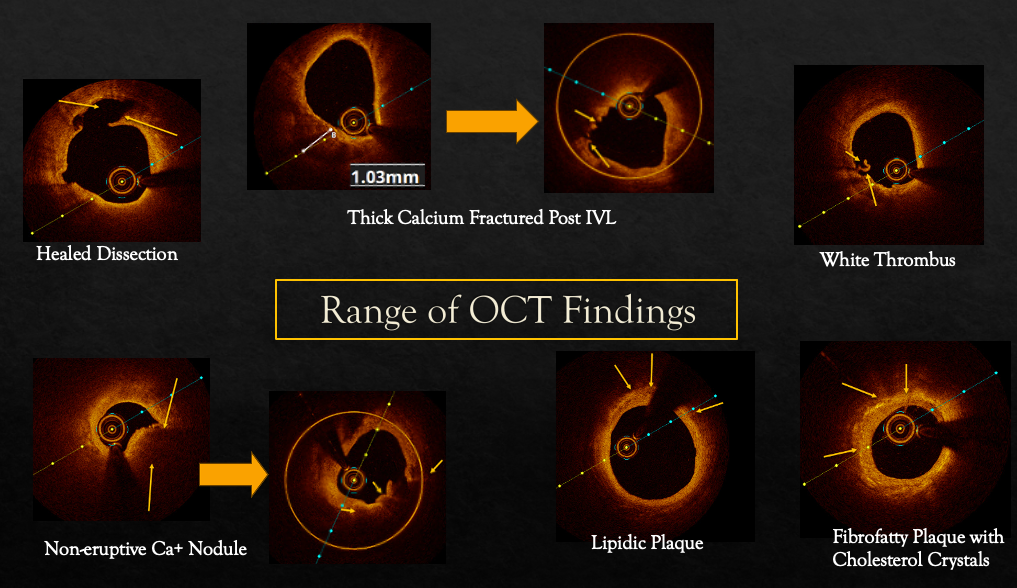
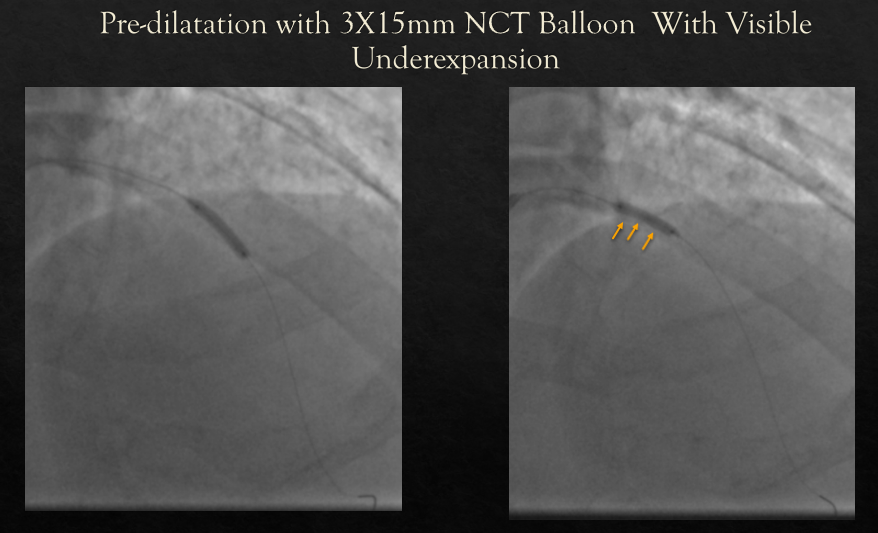
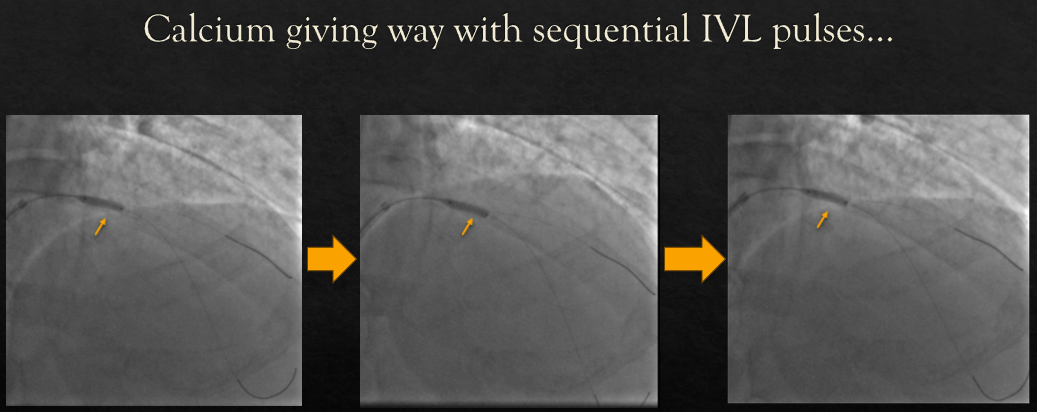
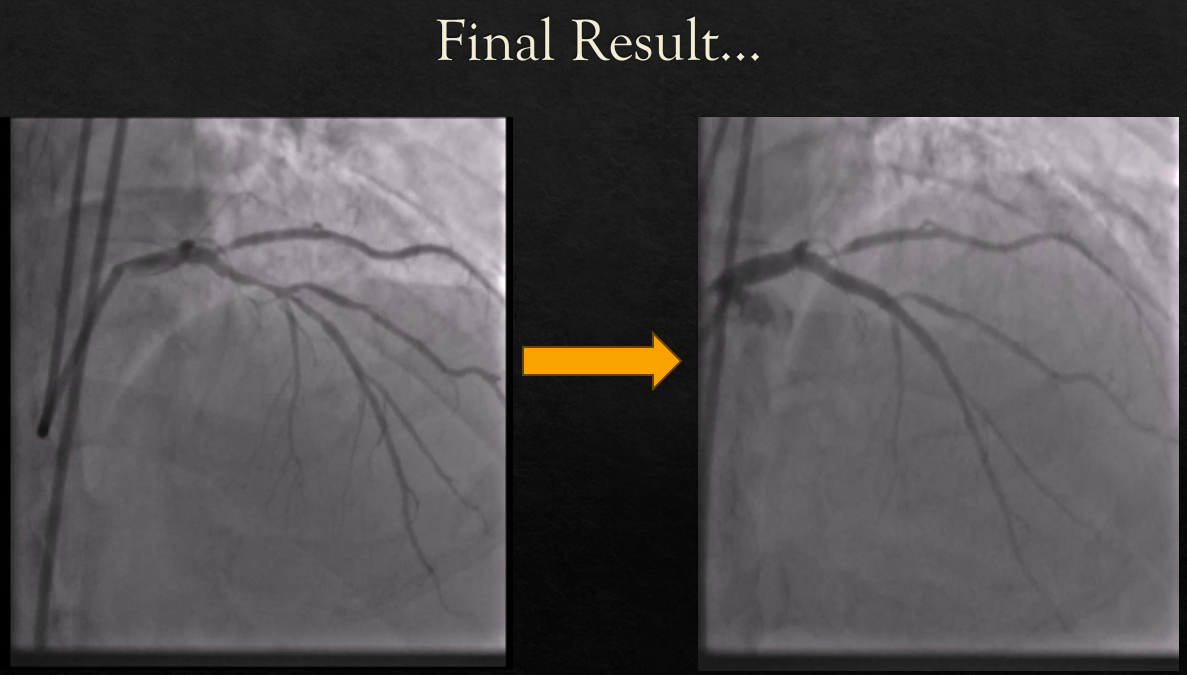
Left Coronary artery was engaged with a 7F XB catheter. Lesion was crossed with a 0.014'' Sion Blue Wire. Initial OCT run revealed a host of findings like healed dissection, thick calcium, thin calcium, a non-eruptive calcium nodule, fibro-fatty and a lipidic plaque. The lesion was pre-dilated with a 3X15mm NC balloon, which did not expand fully at the site of the nodule. Further bed preparation was done with a 3X12mm IVL balloon with pulses around the heavily calcified area. After adequate bed preparation, a 3X38mm DES was implanted and post dilatation was carried out with a 3.5X12mm NC Balloon for an optimal result.
Case Summary
OCT can reveal multiple pathologies in an artery, not immediately appreciated by angiography. Appreciation of the morphology assists in better bed preparation and eventually optimum stent expansion. IVL works in patients with calcium nodule as evidenced in our case, while producing cracks on either side of the summit of the nodule, resulting in collapse of the nodule as a whole and increase in the lumen area. Ideally, calcific lesions should be assessed by the intravascular imaging (preferably OCT) before stent implantation. This is a special learning case due to the variety of OCT findings were found in this case.