
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-188
Nightmare in the Cathlab: A Superficial Femoral Artery Pseudoaneurysm After Transcatheter Peripheral Vascular “Bypass” for Superficial Femoral Artery Chronic Total Occlusion
By Li Ying Yu, Cheng Yu Ko, Cheng-Han Lee
Presenter
Li Ying Yu
Authors
Li Ying Yu1, Cheng Yu Ko2, Cheng-Han Lee3
Affiliation
Ministry of Health and Welfare Tainan Hospital, Taiwan1, National Cheng Kung University Hospital, Taiwan2, Tainan Municipal Hospital, Taiwan3,
View Study Report
TCTAP C-188
Endovascular - Iliac / SFA Intervention
Nightmare in the Cathlab: A Superficial Femoral Artery Pseudoaneurysm After Transcatheter Peripheral Vascular “Bypass” for Superficial Femoral Artery Chronic Total Occlusion
Li Ying Yu1, Cheng Yu Ko2, Cheng-Han Lee3
Ministry of Health and Welfare Tainan Hospital, Taiwan1, National Cheng Kung University Hospital, Taiwan2, Tainan Municipal Hospital, Taiwan3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
This was a 90-year-old man with history of complete AV block, post permanent pacemaker implantation, coronary artery disease, post percutaneous coronary intervention, diabetes mellitus, chronic kidney disease, dyslipidemia, hypertension and old stroke. He was wheelchair-bound and had totally dependent activity of daily life. He suffered from worsening gangrene wound and pain over right big and 2nd toes within 1 month.

Relevant Test Results Prior to Catheterization
Ankle-Brachial index was 0.63 on theright and 0.78 on the left. Clinical diagnosis was right foot critical limb ischemia with Rutherfordcategory 6. There was no improvement despite antibiotcstherapyand he did not want amputation. Serum creatinine was 0.87.
Relevant Catheterization Findings
Angiography from left CFA showed extremely tortuous bilateral iliac arteries. We did right CFA ipsilateral approach instead. Angiogram showed total occlusion from orifice of right SFA with a tapered stump but heavily calcified. It was a long CTO with distal stump at TPT and there was another total occlusion at TPT. ATA was totally occluded. Peroneal artery was left to supply foot.


Interventional Management
Procedural Step
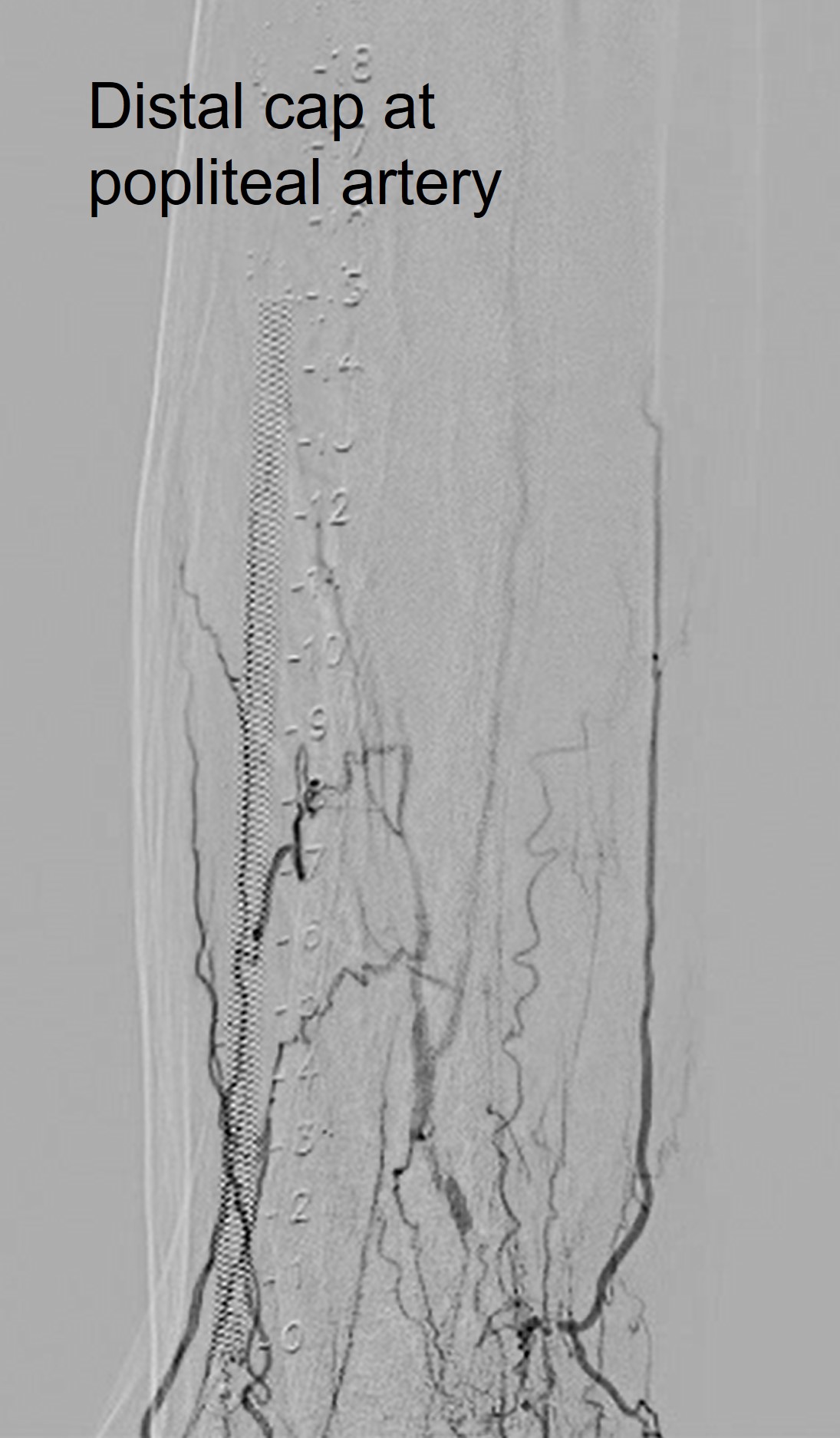
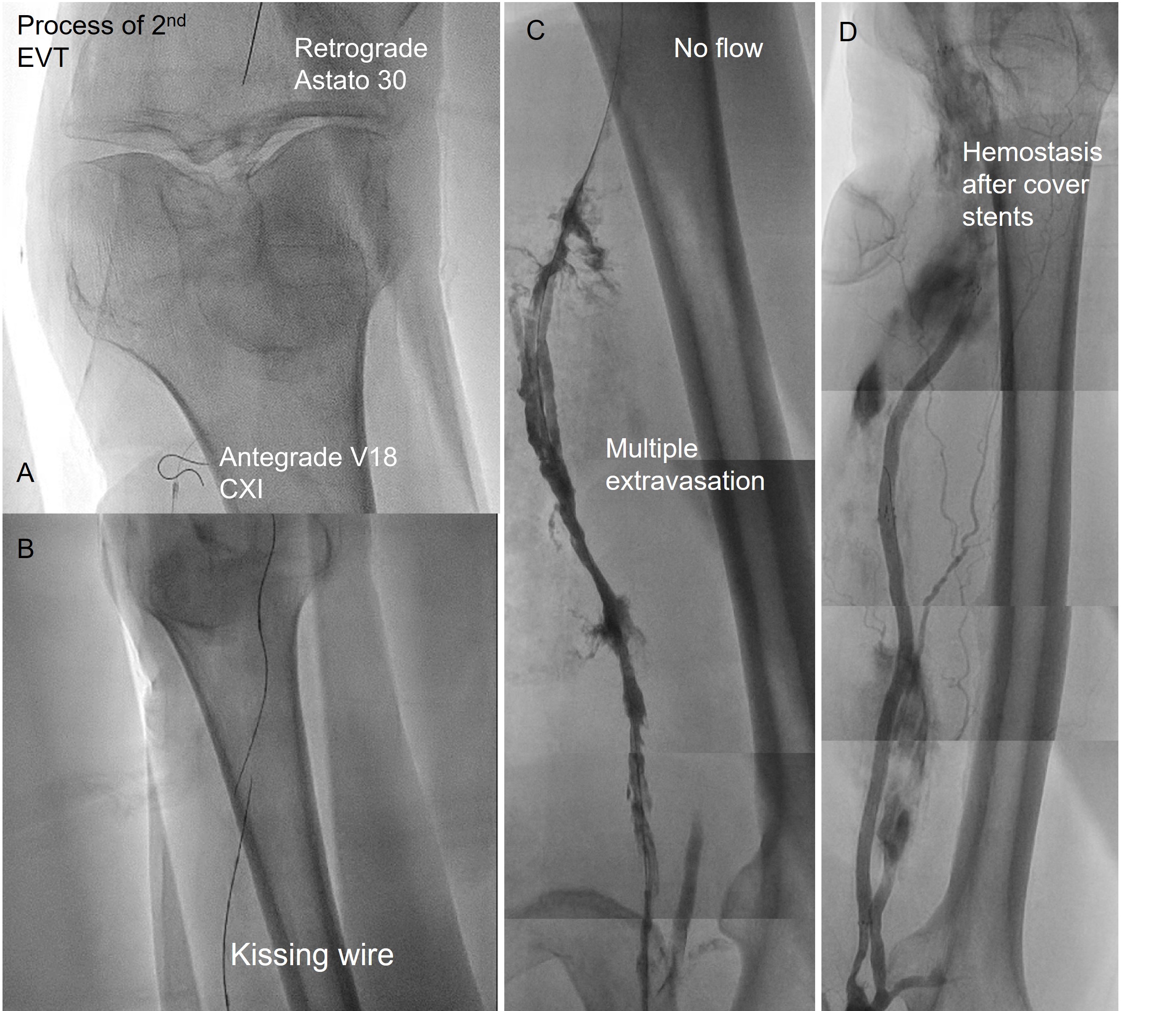
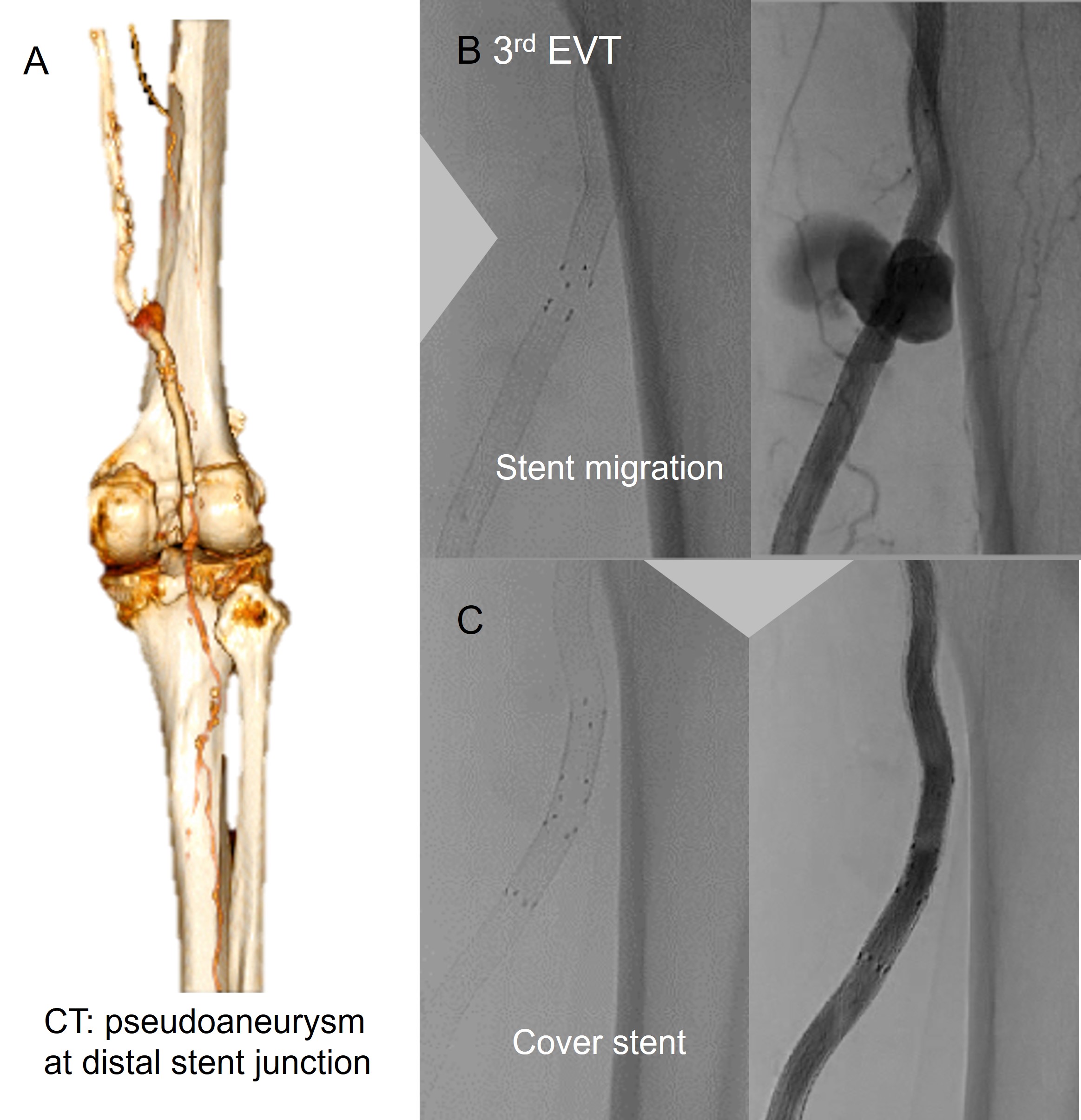
He went through 3 procedures and stayed for 13 days.1st EVT:Do ipsilateral approach at right CFA due to tortuosity of bilateral iliac arteries. We tried antegrade wire escalation ( to Astato 30), knuckle wire technique ( with Hi-torque Connect and CXI) but no progress. And Echo-guided, fluoro-guided distal puncture at peroneal artery failed.2nd EVT:For heavy calcified proximal cap, we used a V18 with microcatheter to do knuckle wire technique and advanced to distal SFA. We did distal puncture at peroneal artery, advanced to popliteal artery and escalated wire to Astato 30 to try penetrate distal cap but failed. R-CART with 4.0 balloon at middle and distal SFA, then externalized retrograde wire. After balloon angioplasty at SFA with 4.0 balloon, angiogram showed multiple extravasations at SFA. The patient developed shock. We did prolonged balloon inflation during resuscitation, but in vain. 3 cover stents were deployed at proximal to distal SFA. No more extravasation.※2 days later, the right thigh swelled and hemorrhagic shock recurred. CT showed a pseudoaneurysm at distal stents junction and the stents were distant from true SFA on transverse cuts. A "bypass" was created.3rd EVT:Stents migrated. A cover stent was deployed to cover pseudoaneurysm. No more bleeding afterward.

Case Summary
It was a "hard" case. To conquer the CTO, we escalated wire and did knuckle wire technique with .018" wire but unexpectedly caused "bypass". To limit dissection, pre-procedural image, like CT would help. While subintimal tracking with knuckle wire technique, a smaller loop made with a softer wire and a microcatheter may do less harm. Intravascular imaging by IVUS would help making sure the wire position and choosing proper size for ballooning.