
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-036
A Case of Successful One-Stage Revascularization by Using Rotablator and Lithotripsy (Rotatripsy) in a Patient With ST-Segment Elevation Myocardial Infarction and Undergoing Chemotherapy for Pancreatic Cancer
By Yasunori Inoguchi, Naoki Hayakawa
Presenter
Yasunori Inoguchi
Authors
Yasunori Inoguchi1, Naoki Hayakawa2
Affiliation
Kanazawa Cardiovascular Hospital, Japan1, Asahi General Hospital, Japan2,
View Study Report
TCTAP C-036
Coronary - Complex PCI - Calcified Lesion
A Case of Successful One-Stage Revascularization by Using Rotablator and Lithotripsy (Rotatripsy) in a Patient With ST-Segment Elevation Myocardial Infarction and Undergoing Chemotherapy for Pancreatic Cancer
Yasunori Inoguchi1, Naoki Hayakawa2
Kanazawa Cardiovascular Hospital, Japan1, Asahi General Hospital, Japan2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
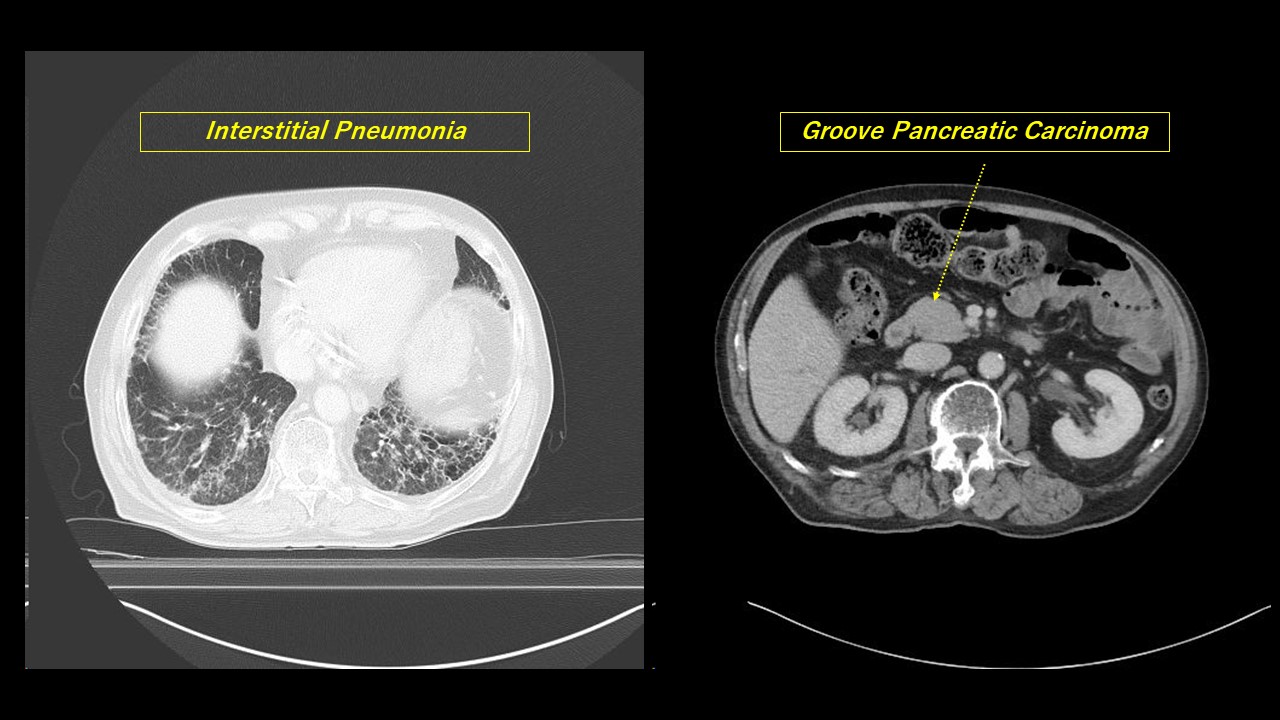
A 75-year-old man had come to our hospital complaining of chest pain from last night. He had underwent chemotherapy with paclitaxel and gemcitabine against unresectable pancreatic cancer for a year in our hospital.His clinical course of cancer had been good but he suffered from interstitial pneumonia induced by side effects of chemotherapy, so his respiratory function had tended to worsen.However, his prognosis had been still expected to be at least over a year at then.
Relevant Test Results Prior to Catheterization
Electrocardiography showed ST elevation remarkably in V1 to V5 inductions.

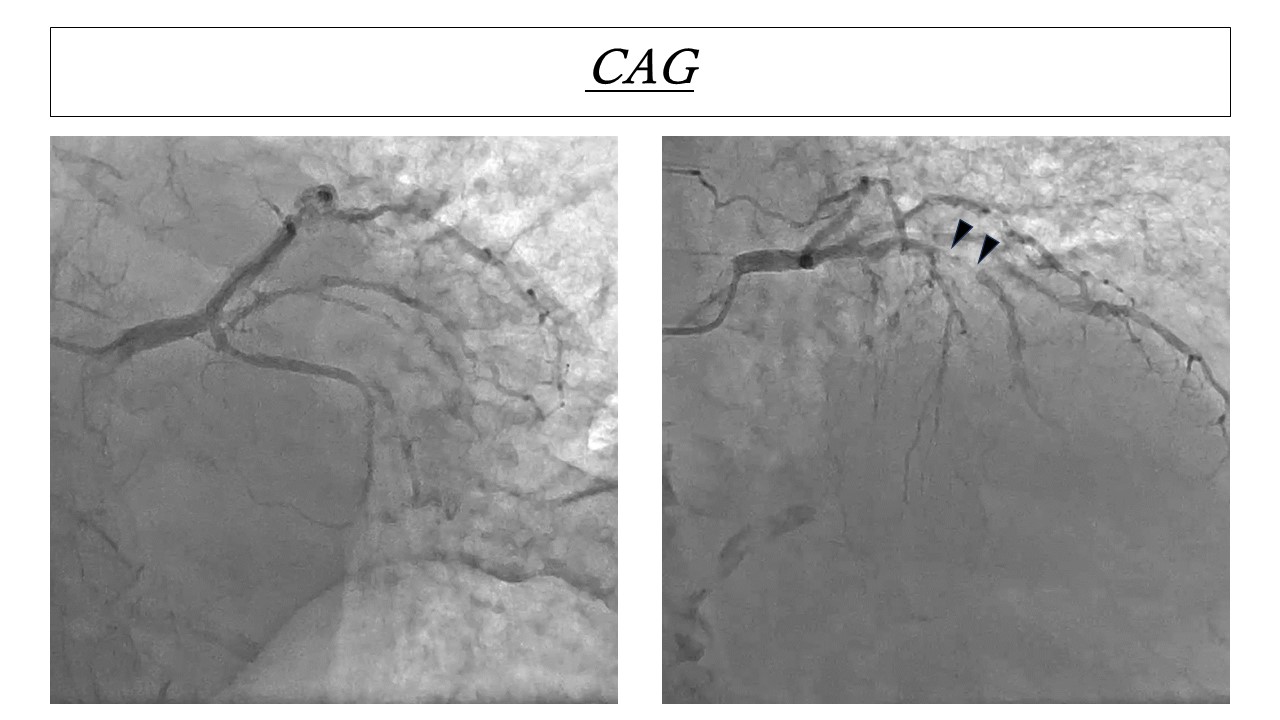
Relevant Catheterization Findings
CAG showed that there was 99% stenosis at seg7 of LAD, 75% stenosis at ramus intermediate, focal 99% stenosis at seg2 of RCA, and flow of LAD was TIMI grade 1.
Interventional Management
Procedural Step
We selected 7Fr Mach1 Q3,5 guiding catheter (Boston scientific, USA).


Case Summary
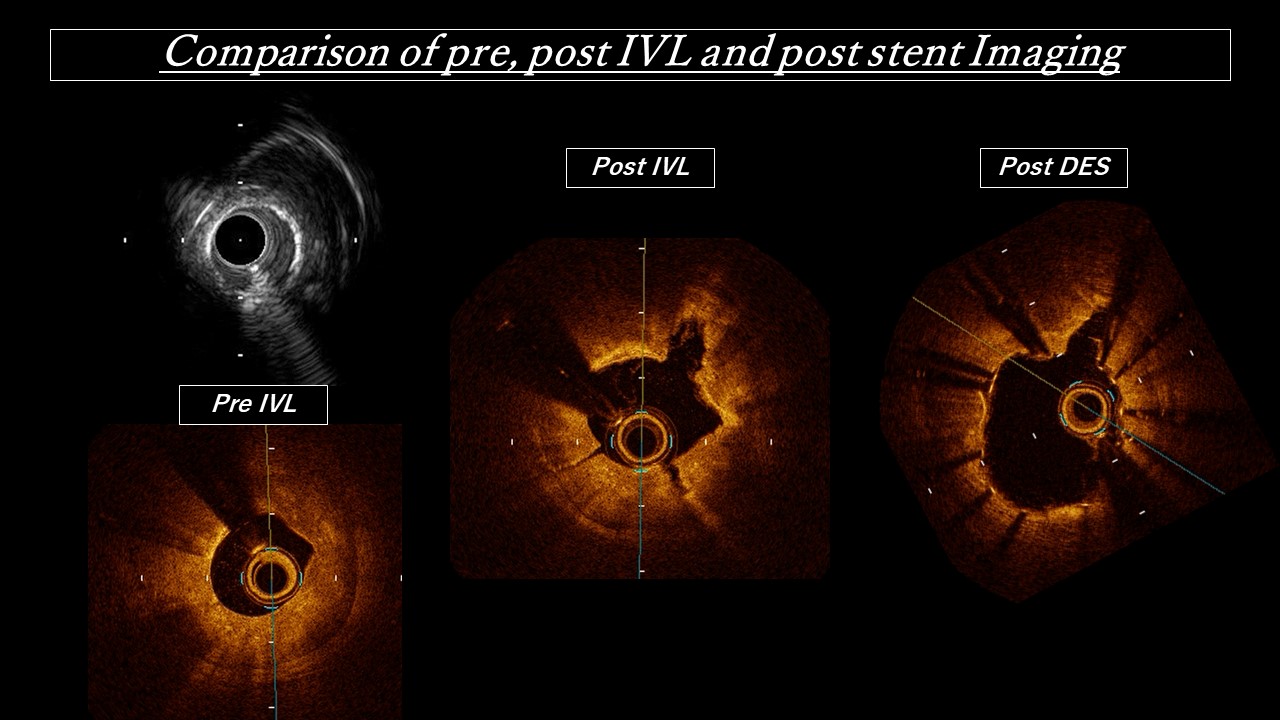
We finally could successful revascularization in a single procedure by combination therapy with rotablator and lithotripsy. Rotablator has advantage of passage performance in calcified lesion, but it might occur slow flow or no reflow phenomenon. On the other hand, lithotripsy has low risk of those complications, but has disadvantage of poor deliver-ability of lithoplasty balloon. Therefore, combination with rotablator and lithotripsy could compensate for shortcoming each other devices, and it makes possible to more effective approach for severe calcified lesions. Especially, it would be one of an effective option or alternative strategy in severe situation like this case.