
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-008
A Management Dilemma: Case of Coronary Artery Ectasia Presenting as ST Segment Elevation Acute Myocardial Infarction in a 56- Year- Old Male
By Ma Victoria Collantes Fernandez, Marrafe Correa, Meliton III Aquines Evangelista, Ronald Santos, Philipp C. Ines
Presenter
Meliton III Aquines Evangelista
Authors
Ma Victoria Collantes Fernandez1, Marrafe Correa1, Meliton III Aquines Evangelista1, Ronald Santos1, Philipp C. Ines2
Affiliation
St. Luke's Medical Center, Philippines1, Philippine Heart Center, Philippines2,
View Study Report
TCTAP C-008
Coronary - ACS/AMI
A Management Dilemma: Case of Coronary Artery Ectasia Presenting as ST Segment Elevation Acute Myocardial Infarction in a 56- Year- Old Male
Ma Victoria Collantes Fernandez1, Marrafe Correa1, Meliton III Aquines Evangelista1, Ronald Santos1, Philipp C. Ines2
St. Luke's Medical Center, Philippines1, Philippine Heart Center, Philippines2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 56-year-old male, without co-morbidities, had sudden squeezing epigastric pain radiating to left chest 6/10 at rest, persisting for two days. Pain increased to 8/10 during defecation. He was treated as STEMI in a nearby hospital and given Aspirin, Clopidogrel, Fondaparinux, ISDN, and Atorvastatin. In our ED, vital signs were stable. Chest pain persisted with score 8/10, but no signs of cardiorespiratory distress. On physical exam, he had clear breath sounds. Other findings are unremarkable.

Relevant Test Results Prior to Catheterization
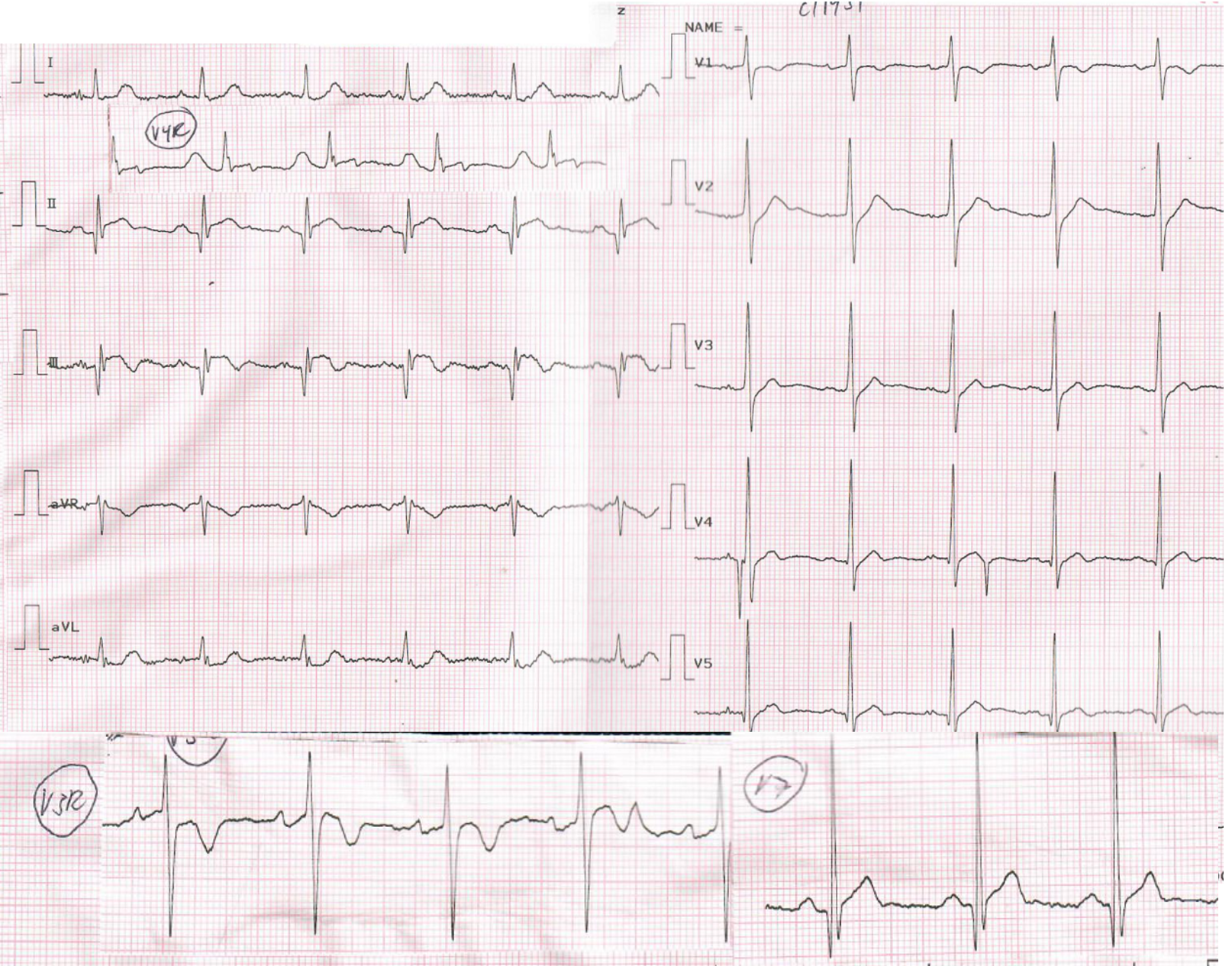
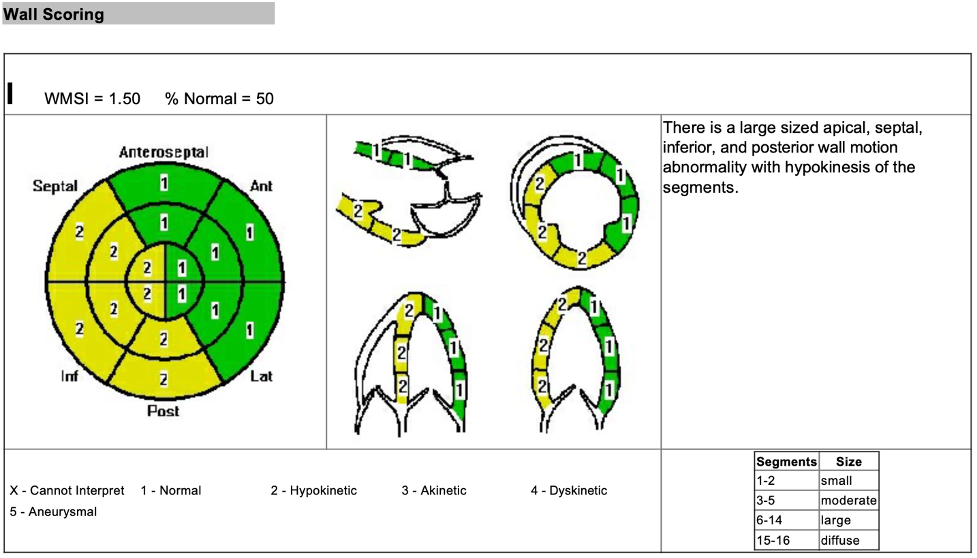
Upon transfer in our emergency department, ECG was done revealing ST segment elevation in leads II, III, and aVF. 2D echocardiography showed hypokinesia in apical, septal, inferior, and posterior walls with ejection fraction of 50.7%. Troponin I was significantly elevated at 155 ng/dl (Normal <25). Other tests done ruled out other differential diagnoses. Chest x-ray did not show signs of congestion. All other parameters including CBC, electrolytes, and renal function, were within normal limits.
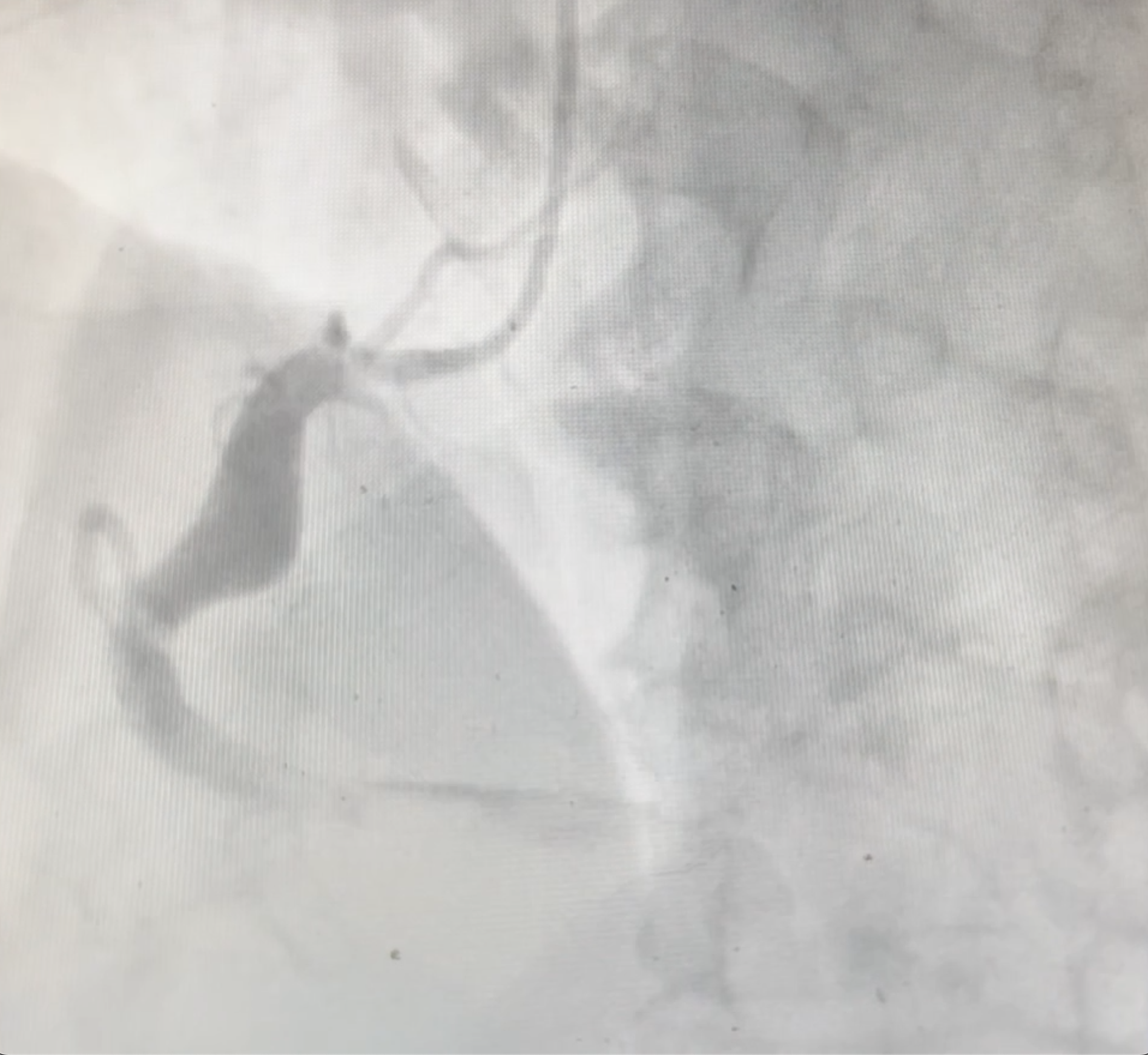
Relevant Catheterization Findings
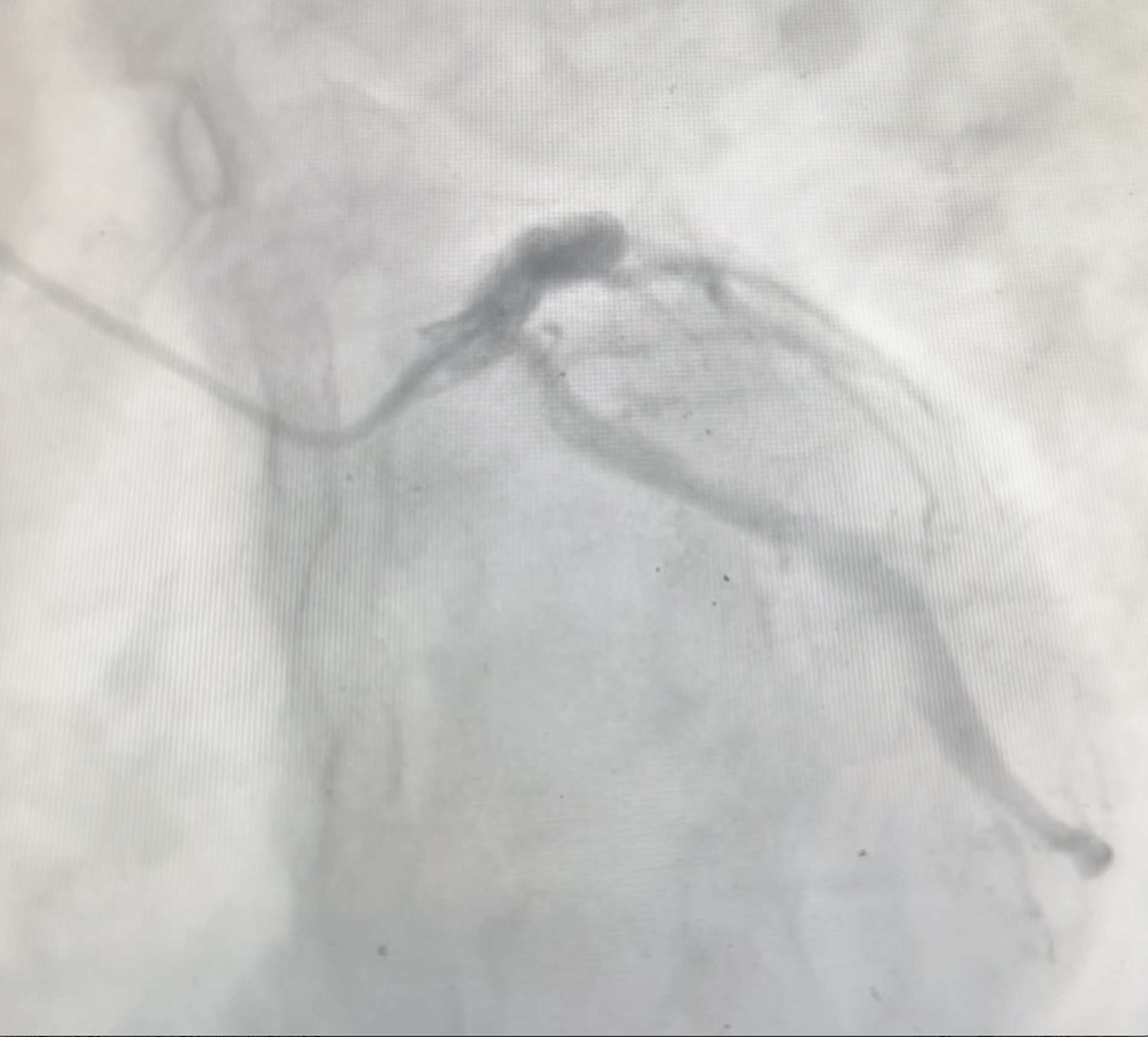
The left main is a normal-caliber vessel that appears disease free. LAD is normal-caliber type III vessel with ectatic segment at late proximal segment and 40% stenosis at late mid segment and minimal luminal irregularities at proximal segment. LCx is a normal- caliber vessel with multiple ectatic segments seen at proximal and mid segments with 50% stenosis seen at the proximal segment. The RCA is a large-caliber vessel with total occlusion at mid segment and ectasia at late proximal segment.

Interventional Management
Procedural Step
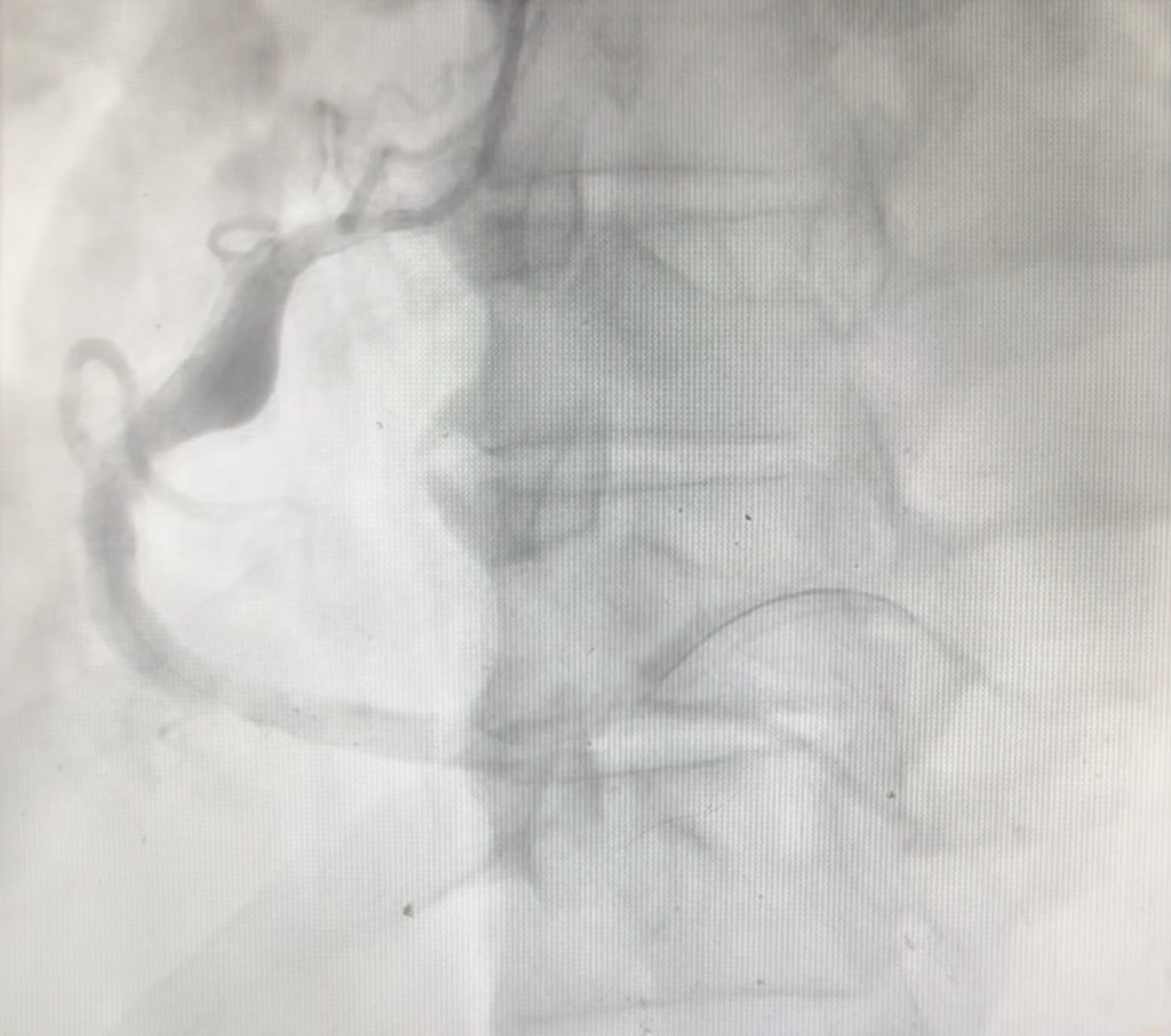
Percutaneous coronary intervention was done at the RCA. A Cordis JR4 6 F guiding catheter was initially used to engage the right coronary ostium. An Asahi sion blue coronary guide wire was advanced into the RCA artery, crossing the lesion at the mid segment with its tip parked at the most distal segment of one of the PLB branches. Balloon pre- dilatation of the distal segment was done and inflated at a maximum of 14 atm (2.78 mm). Another balloon pre-dilatation of the distal segment was done and was inflated at a maximum of 10 atm (3.06 mm). The JR4 6 F guiding catheter was then replaced with a Heartrail JR4 7 F guiding catheter for better support.
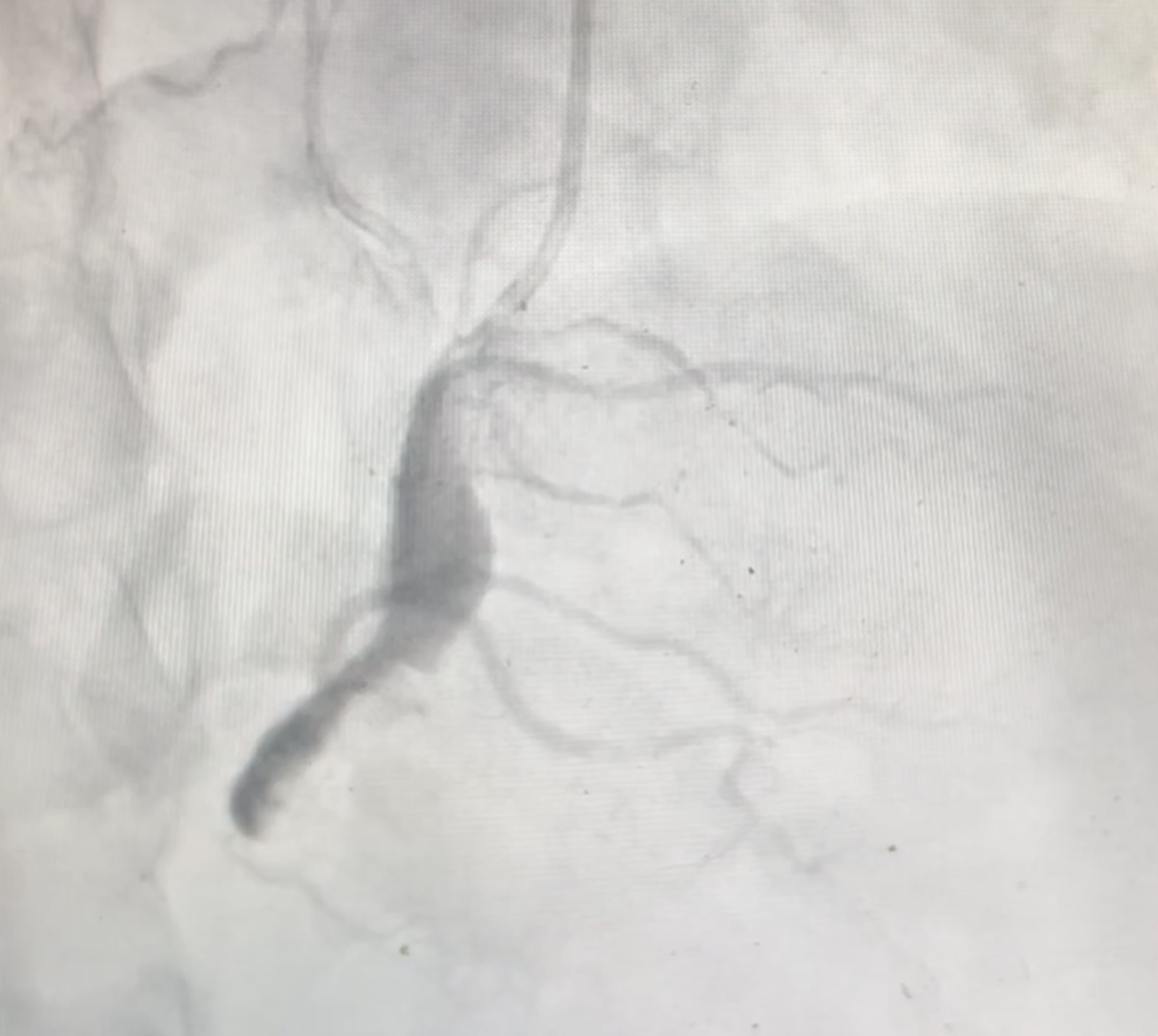
A Runthrough coronary guide wire was then advanced into the RCA artery, crossing the lesion at the mid segment with its tip parked at the most distal segment of one of the PLB branches. Sequential manual aspiration thrombectomy was done multiple times using a Medtronic Export advance aspiration catheter and a Nipro TVAC catheter. Intravascular ultrasound of the mid to distal RCA using a Philips INTRASIGHT with a Refinity catheter via automatic pullback showed a large - caliber vessel with an approximate size of more than 8 mm in diameter. Final angiographic views of the distal RCA showed restoration of TIMI 2 flow in the vessel. There was no evidence of dissection or perforation. Coronary wires and guide catheter were removed and hemostasis was done. DAPT was started and Tirofiban drip was maintained for 24 hours post- PCI.

A Runthrough coronary guide wire was then advanced into the RCA artery, crossing the lesion at the mid segment with its tip parked at the most distal segment of one of the PLB branches. Sequential manual aspiration thrombectomy was done multiple times using a Medtronic Export advance aspiration catheter and a Nipro TVAC catheter. Intravascular ultrasound of the mid to distal RCA using a Philips INTRASIGHT with a Refinity catheter via automatic pullback showed a large - caliber vessel with an approximate size of more than 8 mm in diameter. Final angiographic views of the distal RCA showed restoration of TIMI 2 flow in the vessel. There was no evidence of dissection or perforation. Coronary wires and guide catheter were removed and hemostasis was done. DAPT was started and Tirofiban drip was maintained for 24 hours post- PCI.
Case Summary
PPCI POBA is a viable option to establish blood flow in severely dilated CAE which do not permit stent placement. For CAE associated with ACS, guidelines for ACS- AMI should be followed and on acute management of CAE and STEMI, GP IIb/IIIa receptor antagonists should be used for very high thrombus case or option for large ectasia that do not permit effective stent placement. For CAE complicated with AMI, DAPT is the standard of treatment. Anticoagulant may be added for those with less risk for bleeding and high thrombus burden. The limitation of our management is the absence of RCTs and established guidelines in the diagnosis, management, and follow up angiography, if needed.