
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-191
Successful Bidirectional Approach for Three Successive Total Occlusions From Left Common Femoral Artery to Popliteal Artery
By Yi Pan Li, Cheng Yu Ko
Presenter
Yi Pan Li
Authors
Yi Pan Li1, Cheng Yu Ko1
Affiliation
National Cheng Kung University Hospital, Taiwan1,
View Study Report
TCTAP C-191
Endovascular - Other Endovascular Intervention
Successful Bidirectional Approach for Three Successive Total Occlusions From Left Common Femoral Artery to Popliteal Artery
Yi Pan Li1, Cheng Yu Ko1
National Cheng Kung University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
This 82-year-old man presented with the left first toe pain and redness with gangrene change for 3 days. His underlying diseases included CAD post PCI, moderate AS, ESRD, dyslipidemia, complete AV block post pacemaker implantation and old stroke. He was strated on empiric antibitoics. The plasty surgeon and cardiovascular surgeons were consulted for evluation of amputation and possible revascularization. He refused surgical intervention after consultation. PTA was suggested for revascularization.

Relevant Test Results Prior to Catheterization
The lower limbs CTA showed partial stenoses of bilateral CFA, SFA, popliteal arteries, bilateral peroneal, bilateral anterior and posterior tibial arteries.
Relevant Catheterization Findings
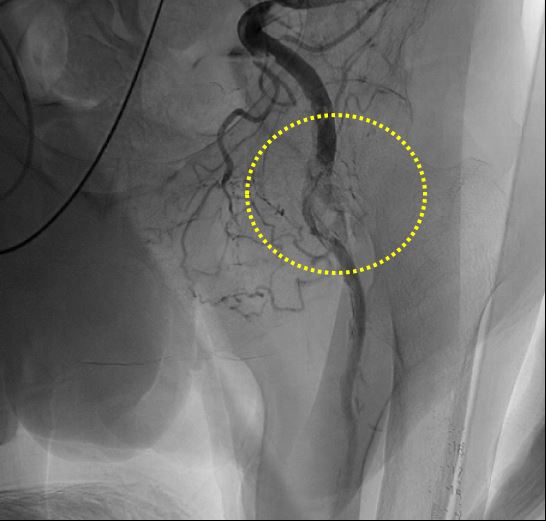
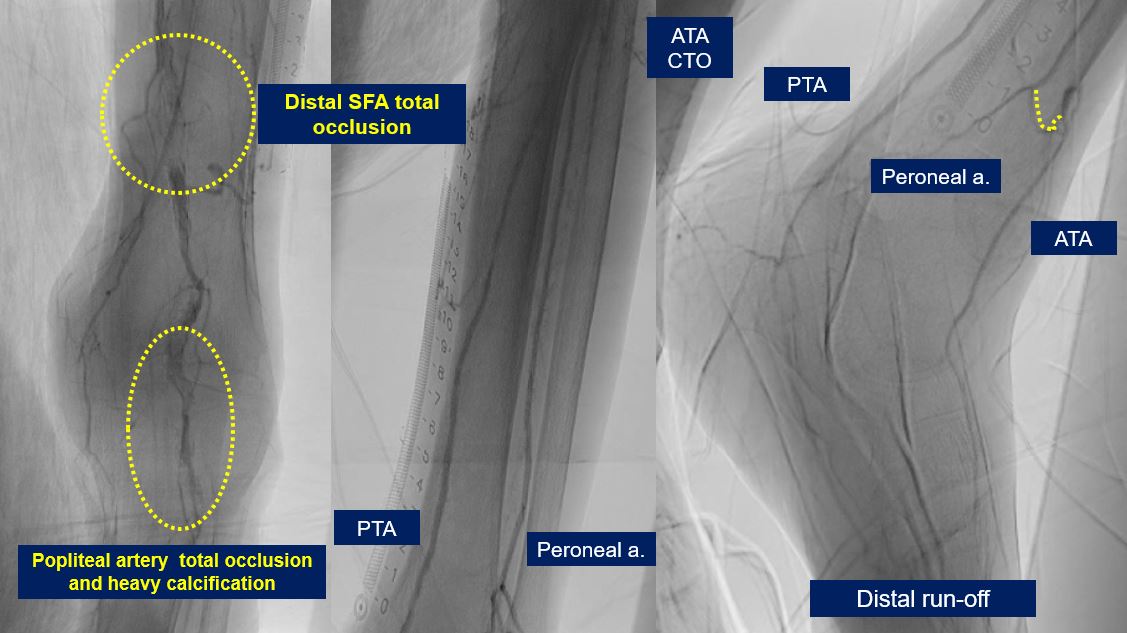
Left side: CIA: very tortuous and diffuse atherosclerosis; EIA and IIA: Diffuse atherosclerosis; CFA: distal total occlusion with a heavy calcified lesion with several collateral to SFA and DFA, SFA: proximal nearly total occlusion, distal SFA total occlusion; DFA: proximal nearly total occlusion; popliteal artery: P2 total occlusion with severe calcified lesion; TPT: diffuse atherosclerosis; ATA: total occlusion; PTA: middle part 80% stenosis; peroneal artery: diffuse atherosclerosis
Interventional Management
Procedural Step
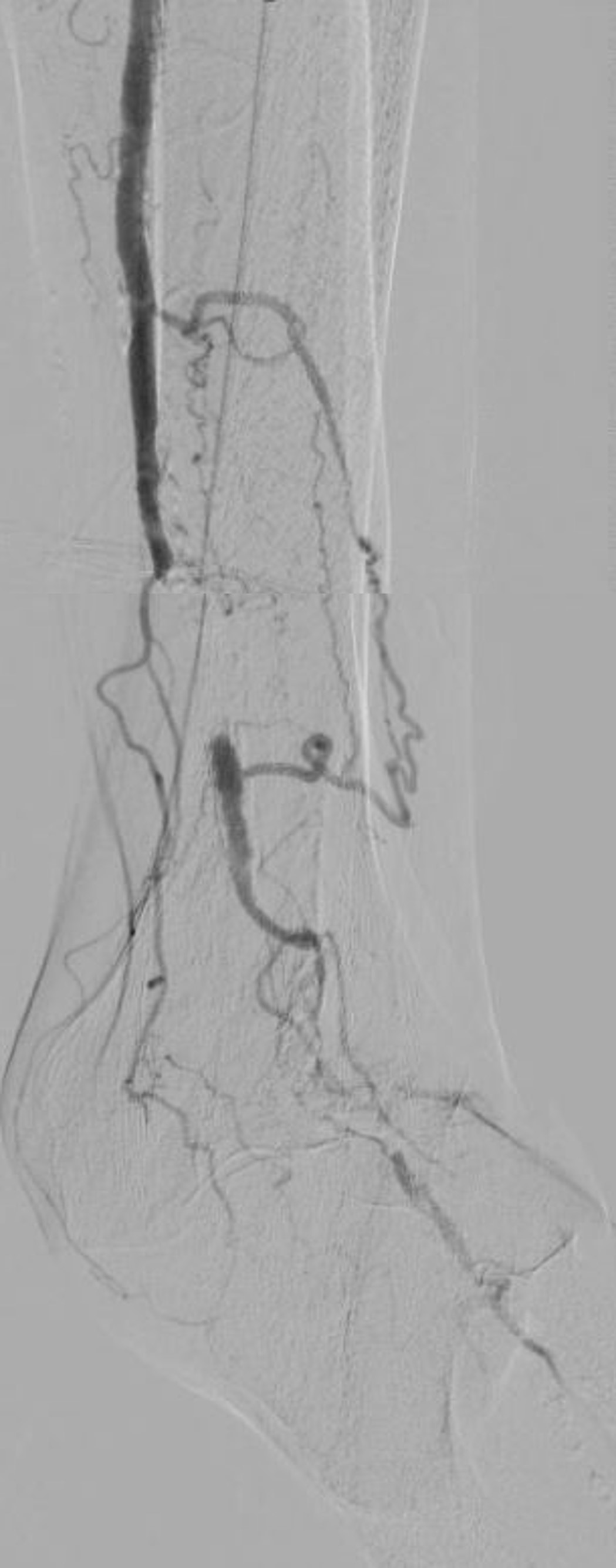
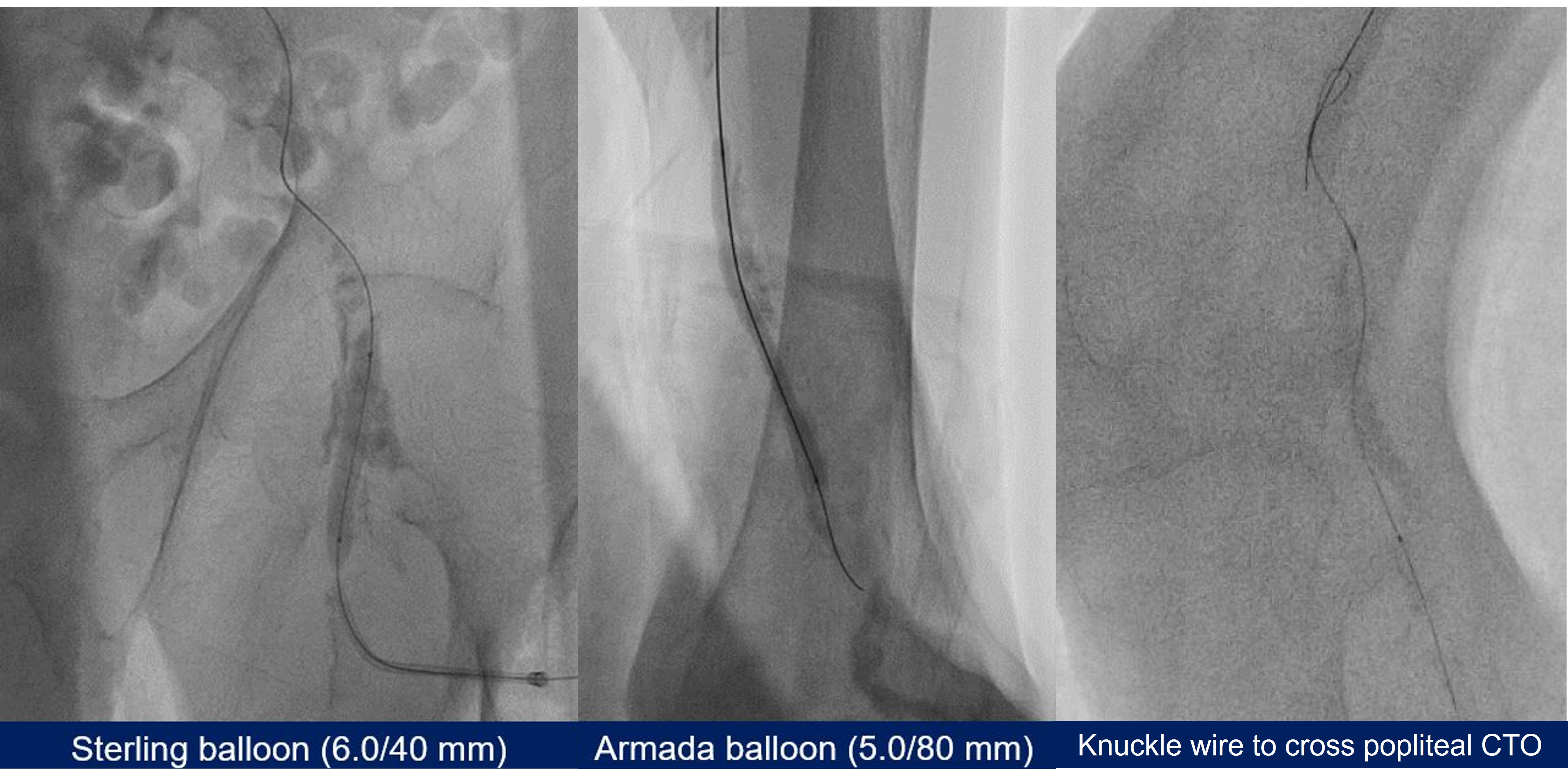
First, the Approach hydro ST wire supported by CXI support catheter passed through the left CFA retrogradely via SFA vascular access. The semicompliance (SC) balloons (5.0/80 mm, 6.0/40mm) were inflated to dilate left CFA. Second, we performed left SFA puncture for ipsilateral antegrade approach. The Astato wire with CXI catheter punctured through the calcified left SFA total occlusive lesion. SC balloon (5.0/80mm) was used to expand left distal SFA. Hypotension occurred, caused by left SFA retrograde sheath site bleeding. We performed prolonged balloon inflation. The retrograde SFA sheath was removed. Hemostasis was achieved thereafter. The V-18 and Astato XS 20 wire failed to go into true lumen of popliteal artery. We started retrograde approach via left PTA. Knuckle wire technique by High-torque Connect wire with CXI catheter successfully passed through the popliteal CTO part. Hypotension occurred again but prolonged inflation couldn't stop bleeding. Therefore, we deployed a covered stent (6.0/40mm) to achieve hemostasis via a new antegrade vascular access from left CFA. After the knuckle wire passed the popliteal CTO, we performed externalization. SC balloon (4.0/80mm) was used to dilate popliteal artery. The other workhorse wire was advanced to left PTA, followed by SC balloon angioplasty (2.0/120mm) for left PTA. The final angiogram showed good flow from left CFA to PTA and peroneal artey. The patient was free from amputation thereafter.


Case Summary
We passed the CFA CTO by retrograde wire escalation with direct wire puncture, crossed the distal SFA CTO by ipsilateral antegrade wiring with direct wire puncture and overcome the popliteal artery CTO by retrograde knuckle wire technique. We used three different approach to beat the three three CTO one by one. At the same time, we resolved the vascular complication by covered stent deployment at SFA. We didn't perform atherectomy and DCB for distal SFA and popliteal artery due to patient's socio-economic status. It's crucial to be familiar with bidirectional approach and several techniques to beat peripheral CTO. To choose different vascular accesses based on the lesions is also important.