
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-010
Extensive Anterior Myocardial Infarction in Young Gentleman With Single Coronary Artery Anomaly
By Chew Fui Lo, Houng Bang Liew
Presenter
Chew Fui Lo
Authors
Chew Fui Lo1, Houng Bang Liew1
Affiliation
Queen Elizabeth II Hospital, Malaysia1,
View Study Report
TCTAP C-010
Coronary - ACS/AMI
Extensive Anterior Myocardial Infarction in Young Gentleman With Single Coronary Artery Anomaly
Chew Fui Lo1, Houng Bang Liew1
Queen Elizabeth II Hospital, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
18-year-old gentleman with no significant past medical history presented with acute chest pain while playing futsal. Aside from being a smoker, he didn't have other cardiovascular risk factors. He denied fever and no chest trauma. There is no history of substance abuse. On examination, he was warm and dry, BP 95/55 mmHg, HR 80 bpm, regular, S1 and S2 heard, no additional heart sound or murmur heard. Other examinations were unremarkable.
Relevant Test Results Prior to Catheterization
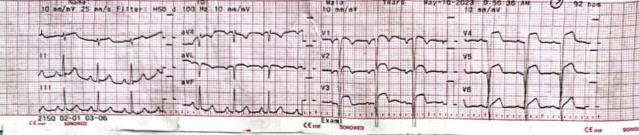
ECG showed sinus rhythm, normal axis, Q wave, and ST elevation over V1-V6. TTE shows LVEF was impaired, 30–35%; valves were normal; no evidence of aortic dissection or aneurysm; no pericardial effusion.CXR was normal.CKMB was raised to 502 IU/L.Hemoglobin was 13 g/dl.Creatinine was 80 umol/l, and eGFR was 109 ml/min/1.73 m2.
Relevant Catheterization Findings
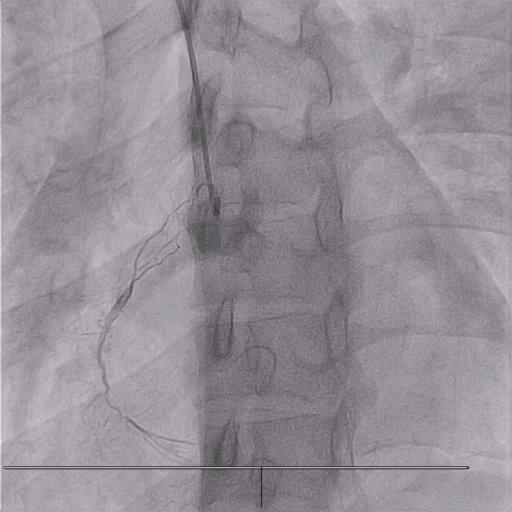
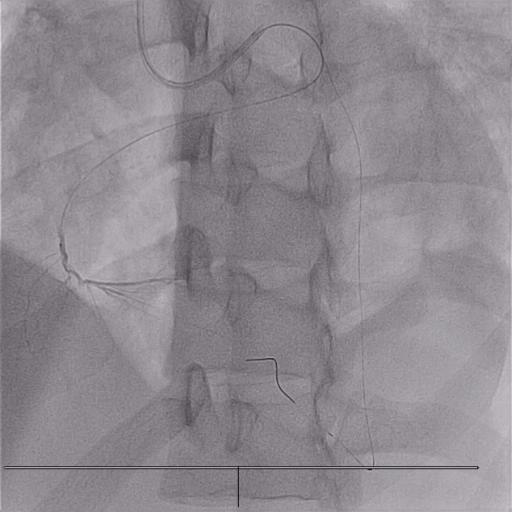
LM: Normal.Lcx: Co-dominant. Normal.LAD: Proximal 70–80% stenosis due to thrombus. RCA: Dual supply. One was from proximal LAD, and another was from the ostium of the right cusp, which degenerated because of competitive flow from proximal LAD.

Interventional Management
Procedural Step
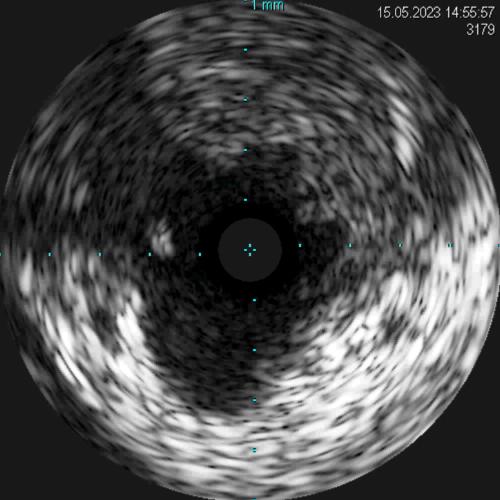
The procedure was done via transradial approach; 6Fr EBU 3.5 was used to engage the left coronary artery. BMW guidewires were passed to the distal LAD and to the RCA, which originated from the proximal LAD. A microcatheter was passed to the RCA, and selective injection was done via the microcatheter to confirm PDA. IVUS was performed to confirm the presence of thrombus at the proximal LAD, which caused stenosis. In view of TIMI 3 flow to distal LAD, PCI was deferred. Triple therapy was planned, and a surveillance coronary angiography was scheduled. One month later, the patient was electively admitted for surveillance angiography. He was clinically well; NYHA class I, CCS class I. Repeated coronary angiography showed the thrombus at the proximal LAD had resolved. After coronary angiography, we concluded that the thrombus formation was due to aneurysmal LAD that caused acute myocardial infarction in this young gentleman. The flow to LAD was restored after the administration of fibrinolytic agent, and the thrombus dissolved after one month of anticoagulant. He is currently on guidelines directed medical therapy for heart failure and lifelong novel oral anticoagulant for secondary prevention of myocardial infarction.

Case Summary
This is a case of a single coronary artery anomaly with aneurysmal LAD which predisposes to thrombus formation and presenting as anterior MI. Anomalous origin of RCA is a rare congenital defect, whereas RCA originates from LAD, like in our case, is even rarer. Medical therapy and defer PCI strategy for thrombus due to aneurysmal coronary artery, especially in the presence of TIMI 3 antegrade flow, is a reasonable option and this group of patient will need lifelong anticoagulant for secondary prevention of myocardial infarction.