
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-129
Retrieval of Double Dislodged Deformed Stent During Primary Angioplasty : A Challenging Case
By Susanta Pradhan
Presenter
Susanta Pradhan
Authors
Susanta Pradhan1
Affiliation
Utkal Hospital, India1,
View Study Report
TCTAP C-129
Coronary - Complication Management
Retrieval of Double Dislodged Deformed Stent During Primary Angioplasty : A Challenging Case
Susanta Pradhan1
Utkal Hospital, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 60 year Male admitted with Acute Inferior wall STEMI with CHB and acute kidney injury. His coronary risk factors were Diabetes & Hypertension. Physical examination revealed Blood pressure was 90/60 mm Hg and HR-50/min .His baseline ECG showed ST elevation in inferior leads with CHB and Echo revealed Hypokinesia in RCA territory with LVEF of 45% with RV dysfunction.

Relevant Test Results Prior to Catheterization
His blood gas analysis showed metabolic acidosis. Serum creatinine was 2.2 mg/dl ,serum sodium was 132 mg/dl, serum potassium was 5.1 mg/dl, blood sugar was 326 mg/dl & Troponin I was 27017 ng/L. Patient was immediately underwent coronary angiography with temporary pacemaker support.
Relevant Catheterization Findings
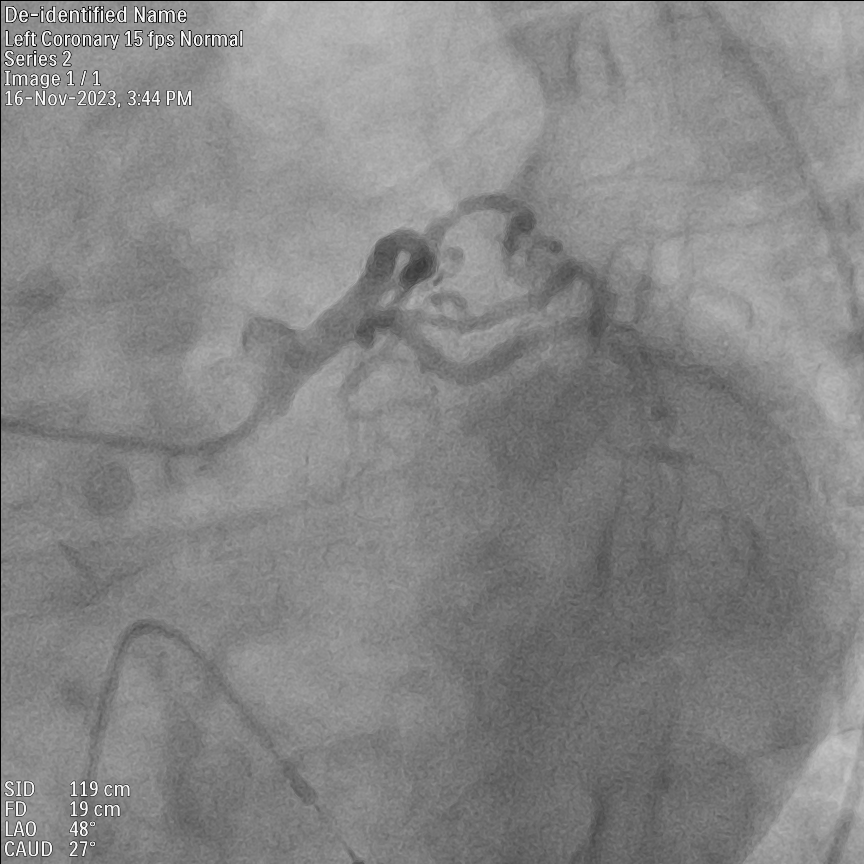
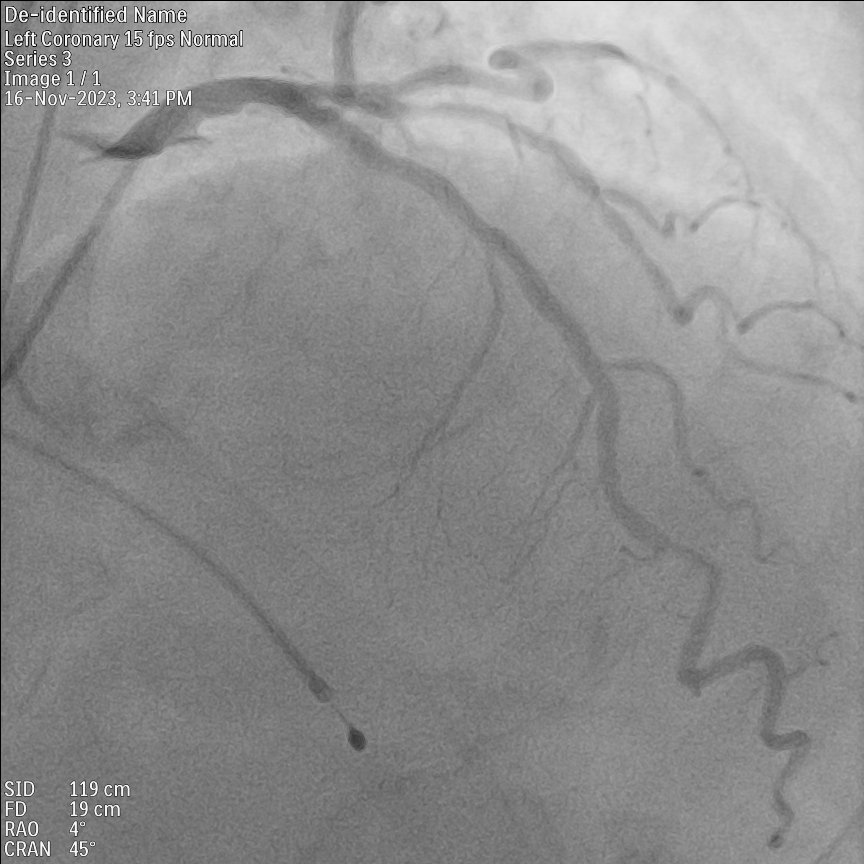
Baseline CAG- Angiography done through right femoral artery approach.1. LMCA was normal, LAD showed minor disease in mid segment, LCX was normal .2.RCA was 100% occlusion from proximal segment.
Interventional Management
Procedural Step
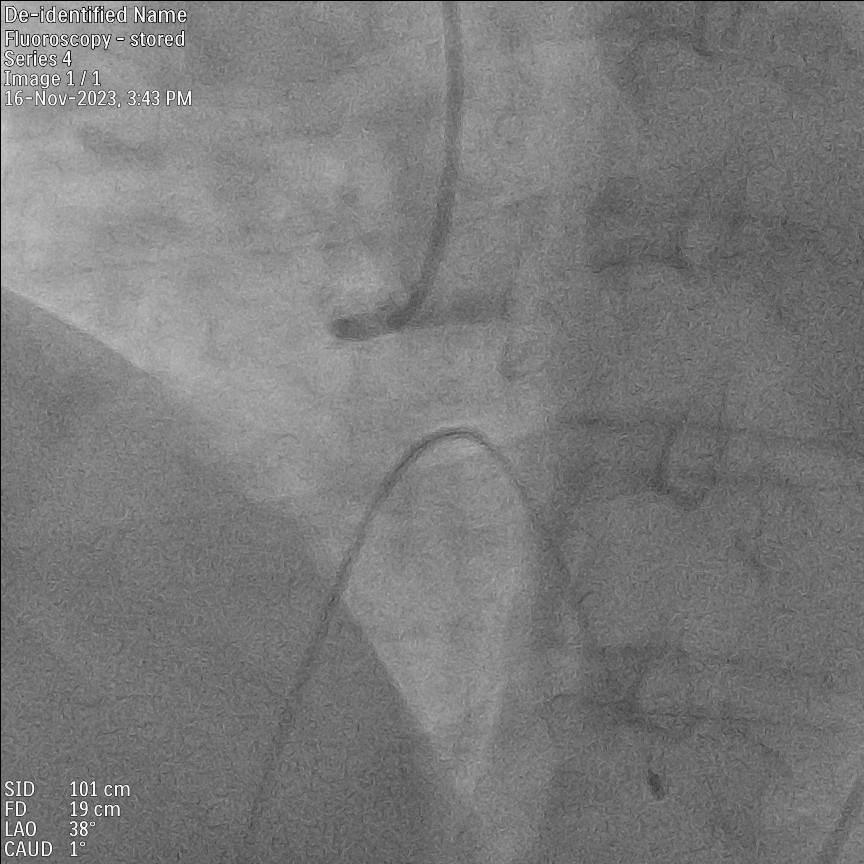
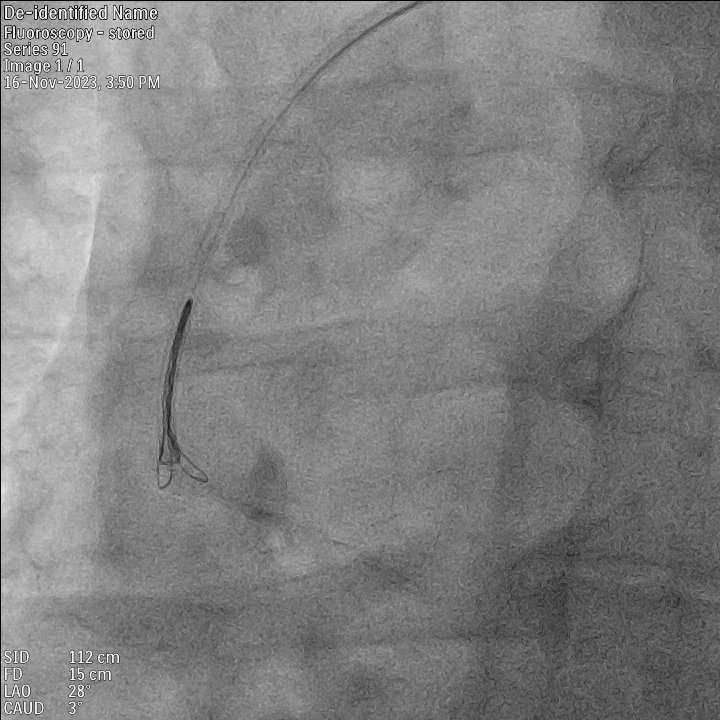
Right Coronary artery was engaged with 6F JR 1 guiding catheter through right femoral artery approach. The RCA lesion was crossed with Runthrough NS Floppy 0.014 guidewire and the proximal lesion was predilated with 3.0x12 mm NC trek balloon. After careful checking a drug eluting stent of 4.0x28 mm was deployed from ostio-proximal RCA. The stent was post dilated with 4.0x12 mm NC trek balloon at 20 atmospheres. After proximal stent deployment the lesion in distal RCA looks more significant which was predilated with 3.0x12 mm NC trek balloon. Than planned to deploy distal RCA with 3.5x32 mm drug eluting stent. However the stent found difficult to cross the proximal deployed stent and also had difficult to pull-back. In addition an attempted forced pullback, it was stripped off from the balloon and remained hanging in Aorta from RCA ostium. As the dislodged stent was over the guide wire, so tried to catch it with 2.5x12 mm inflated balloon half within the guiding catheter. Although it caught the dislodged stent but during retrieval all came out along with guidewire and stent remained hanging in Aorta. Then with the help of Trifoliate EN Snare 6F (9mm-15mm) the dislodged stent was caught. In the process of retrieval hanging stent and previous deployed stent came out with both stents intertwined between them through femoral artery. Finally, the RCA was deployed with 3 overlapping drug eluting stents of sizes 3.5x24 mm,3.5x28 mm &4.0x44 mm from distal to proximal successfully.


Case Summary
Coronary stent dislodgement is an uncommon occurrence during coronary angioplasty and often associated with significant morbidity and mortality. Good alignment between the guiding catheter and coronary ostium is required to avoid crossing difficulties particularly when previous stent was deployed from ostium. Retrieval of deformed and dislodged stent can be done with different manoeuvres including snaring. But in our case as both stents intertwined between them, so during retrieval with snare both stents were came out. After retrieval, patient was successfully managed with three overlapping drug eluting stents from distal to proximal RCA.