
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-106
Retrieval of a Partially Degloved and Distorted Coronary Stent – The Snare to the Rescue
By Boon Cong Beh, Shawal Faizal Mohamad, Mohd Asyiq Al-Fard Bin Mohd Raffali, Noor Diyana Binti Mohamad Farouk, Hamat Hamdi Che Hassan
Presenter
Boon Cong Beh
Authors
Boon Cong Beh1, Shawal Faizal Mohamad1, Mohd Asyiq Al-Fard Bin Mohd Raffali1, Noor Diyana Binti Mohamad Farouk1, Hamat Hamdi Che Hassan1
Affiliation
Hospital Canselor Tuanku Muhriz UKM, Malaysia1,
View Study Report
TCTAP C-106
Coronary - Complication Management
Retrieval of a Partially Degloved and Distorted Coronary Stent – The Snare to the Rescue
Boon Cong Beh1, Shawal Faizal Mohamad1, Mohd Asyiq Al-Fard Bin Mohd Raffali1, Noor Diyana Binti Mohamad Farouk1, Hamat Hamdi Che Hassan1
Hospital Canselor Tuanku Muhriz UKM, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
59 years old gentleman with co-morbidities of long-standing diabetes mellitus, hypertension, dyslipidemia, previous history of right shoulder joint replacement post trauma and peripheral vascular disease, who admitted for infected left diabetic foot ulcer, complicated with NSTEMI in failure. Appropriate antibiotic was started and subsequently done wound debridement. Initially he was on medical therapy for his NSTEMI.

Relevant Test Results Prior to Catheterization
His highest serum Troponin I level was 8157 pg/mL with serial ECG changes noted T waves inversion in lead III and aVF (evolving changes compare to admission ECG). Chest radiograph showed cardiomegaly with congested lung fields.
Relevant Catheterization Findings
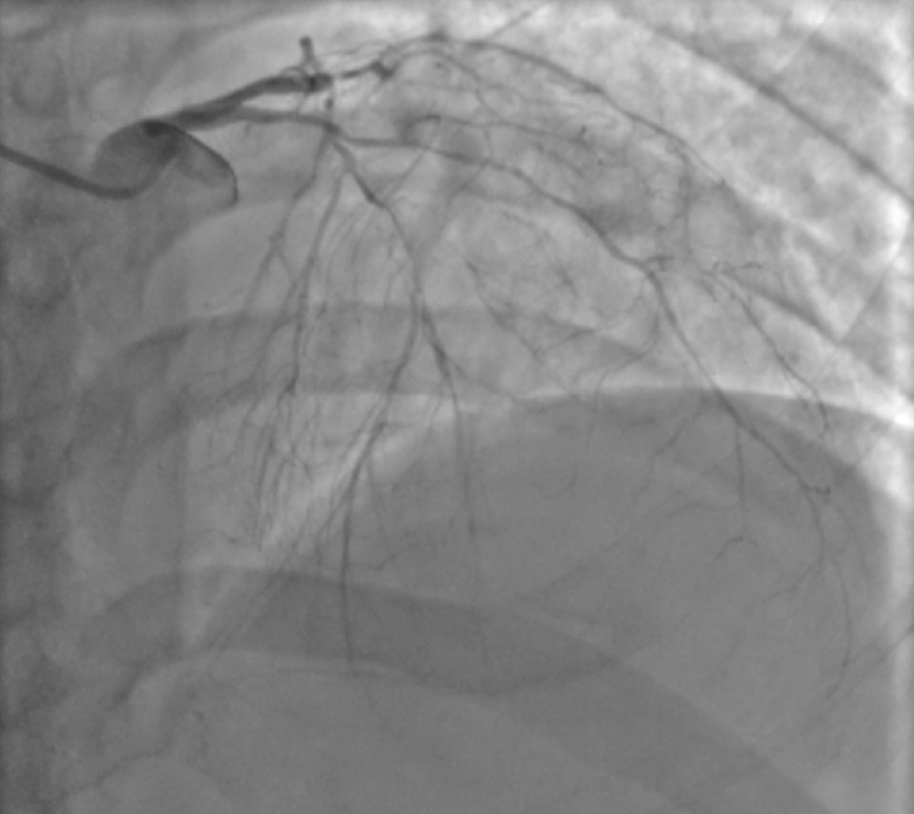
After infection was treated, he was scheduled for coronary angiogram which showed severe diffuse triple vessels disease. We decided for intervention of RCA in view of ECG changes and for medical therapy for the LAD and LCx (which were diffusely disease)

Interventional Management
Procedural Step
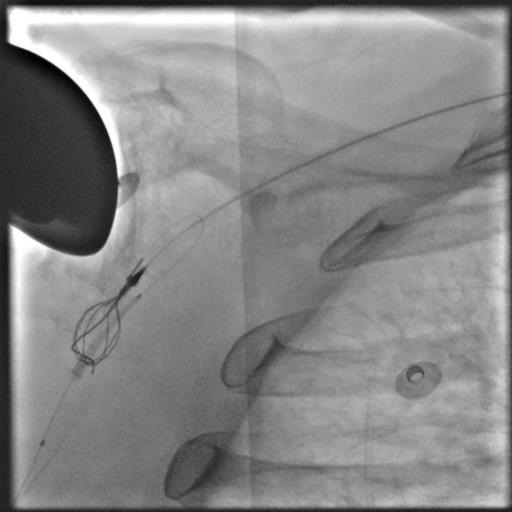
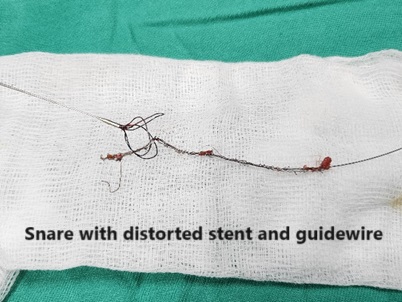
Right radial artery accessed, 6Fr JR 3.5 guide catheter to engage RCA. Sequential predilatation of mid-proximal RCA with NC balloon 2.5x15mm, however, noted proximal segment non-flow limiting dissection. Mid-RCA was treated with drug coated balloon (DCB) 2.5x30mm (high pressure for 1 minute). Subsequently drug eluting stent (DES) was position at proximal RCA overlapped with previous DCB. While adjustment of the stent position, noted the proximal end of the undeployed stent was distorted/crumpled longitudinally and degloved partially (possible due to non-coaxial of guide catheter edge and stent near the ostial RCA). However, unsuccessful removal of the distorted/partially degloved/undeployed stent via the guide catheter/radial sheath. 7Fr right femoral sheath with 260mm guidewire introduced till descending aorta and subsequently snare catheter introduced till the right axillary artery to snare the degloved/distorted stent (partially inflated the balloon for loosen of the distorted stent from the balloon) together with the guidewire removed completely through the right femoral artery puncture site. Adequate compression of the puncture site and heparin reversal with Protamine Sulphate to prevent hematoma/bleeding. 1 week after the index procedure, patient underwent successful stage PCI of proximal RCA with DES 3.0x32mm (nominal) and further optimised with NC balloon 3.5x15mm (nominal). He was discharged well from ward. Follow up in clinic 1 month, he remained asymptomatic.

Case Summary
This case illustrate a successful retrieval of partially degloved and distorted undeployed coronary stent using snare catheter via femoral approach. This is a rare condition where collision between the non-coaxial engagement of guide catheter edge and undeployed stent during manipulation of the stent near ostial coronary artery causing the distorted/crumpled/partially degloved stent. Precaution during ostial coronary manipulation of stent is important to avoid this unwanted event.