
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-035
Challenging Case Report: PCI for Severe Calcified Lesion Using Rotational Atherectomy Device via the SVG Bypass
By Yohei Oishi, Yuzo Akita, Kenta Uemura, Kota Fujihara
Presenter
Yohei Oishi
Authors
Yohei Oishi1, Yuzo Akita1, Kenta Uemura1, Kota Fujihara1
Affiliation
Osaka Saiseikai Izuo Hospital, Japan1,
View Study Report
TCTAP C-035
Coronary - Complex PCI - Calcified Lesion
Challenging Case Report: PCI for Severe Calcified Lesion Using Rotational Atherectomy Device via the SVG Bypass
Yohei Oishi1, Yuzo Akita1, Kenta Uemura1, Kota Fujihara1
Osaka Saiseikai Izuo Hospital, Japan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 80’s year-old male on hemodialysis was admitted to our hospital because of chest pain while hemodialysis. 5 years prior to admission, He had coronary bypass surgery because of effort angina (left internal thoracic artery (LITA)-LAD, saphenous vein graft (SVG)-mid RCA, SVG-diagonal artery-obtuse marginal branch (OM)). At that time, the ostium of RCA was severe stenosis with calcification, not CTO lesion. His coronary risk factors included diabetes, hypertenison and dyslipidemia.
Relevant Test Results Prior to Catheterization
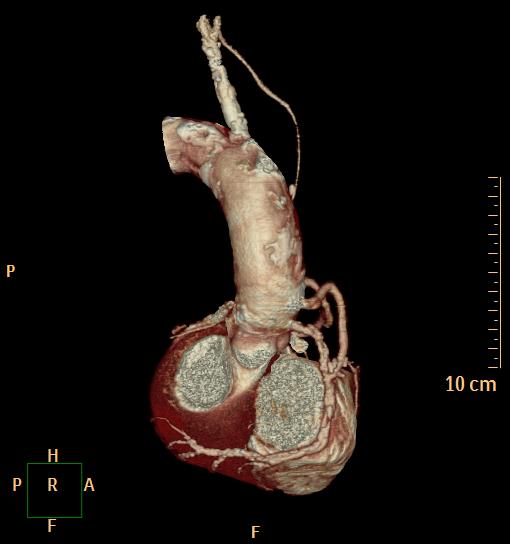
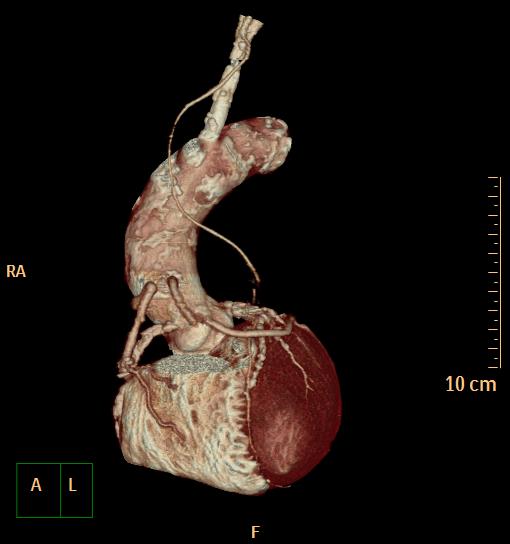
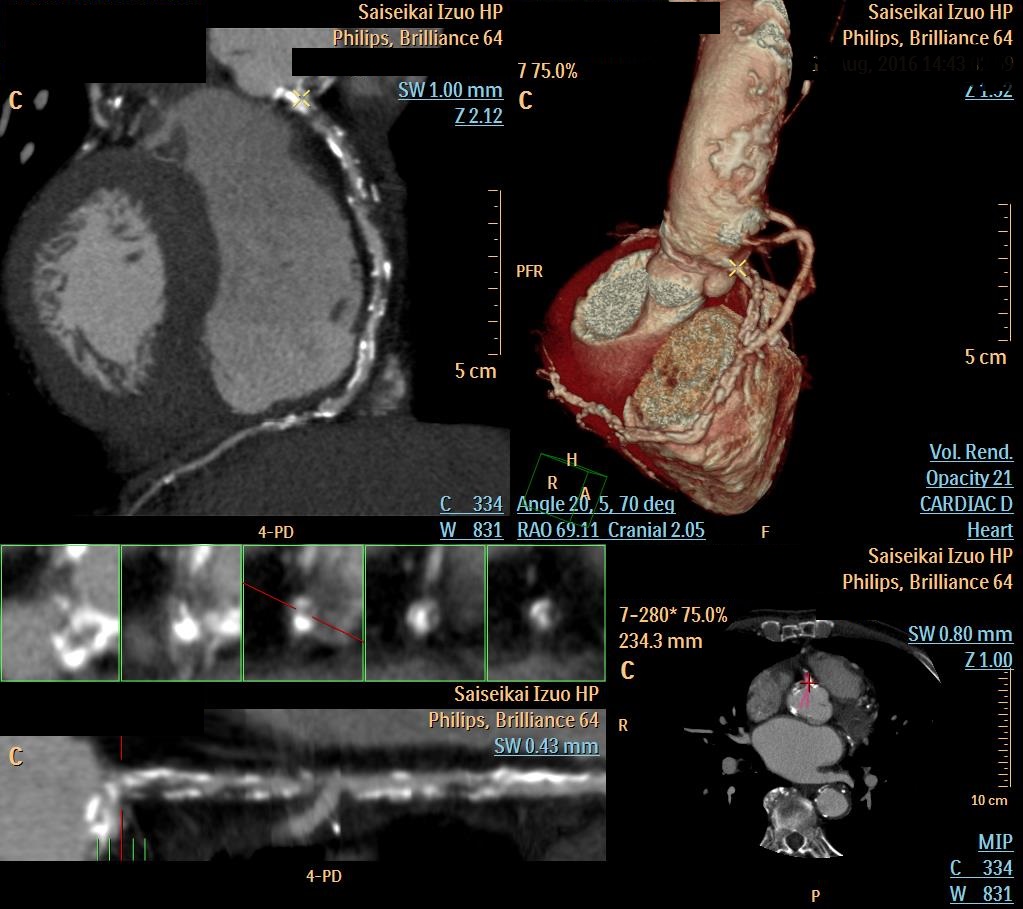
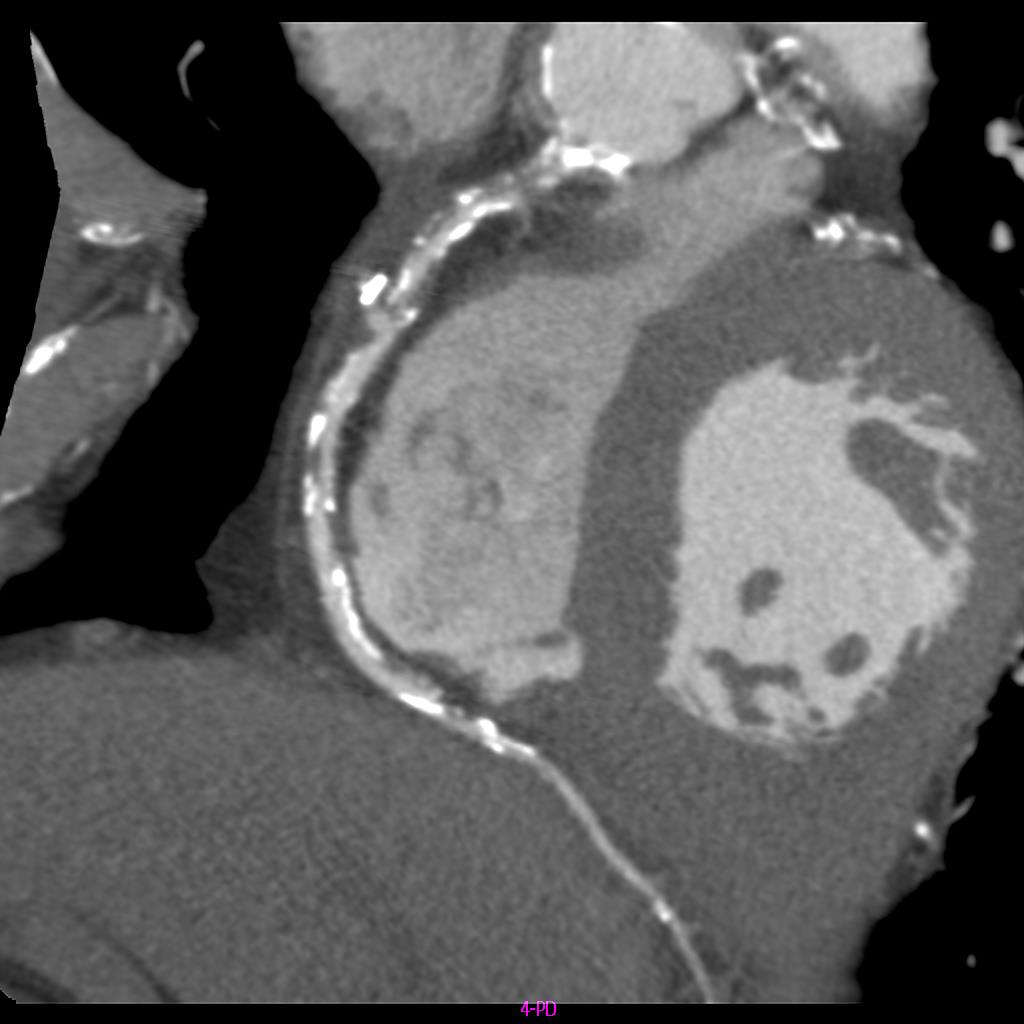
ECG showed pacemaker rhythm, so we didn’t estimate ST change. Cardiac echo showed that Ejection Fraction (EF) was 51.0%, and no asynergy. Coronary CT showed that distal RCA was severe stenosis with strong calcification though bypass graft was patent.
Relevant Catheterization Findings
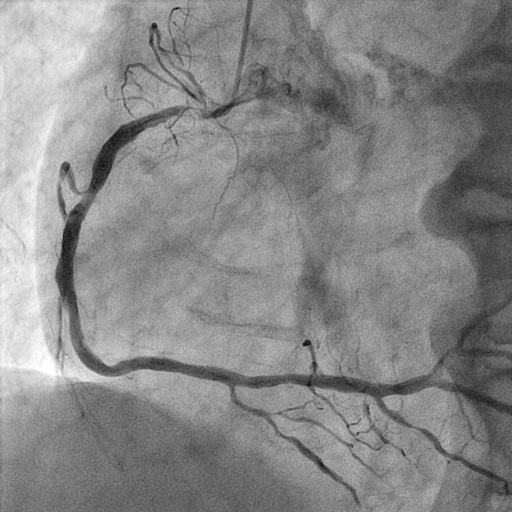
RCA and Cx were occluded at the ostium. LM-LAD and mid LAD were severe stenosis with strong calcification. LITA-LAD, SVG-mid RCA and SVG-diagonal branch-OM were patent and blood flow was good. But severe stenosis with strong calcification was observed in distal RCA, the distal part of the bypass anastomosis.

Interventional Management
Procedural Step
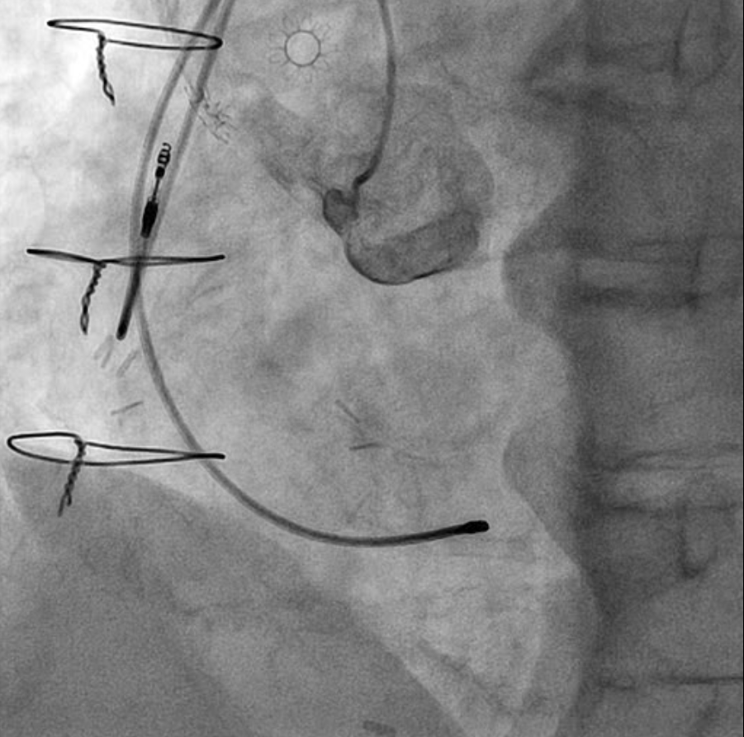
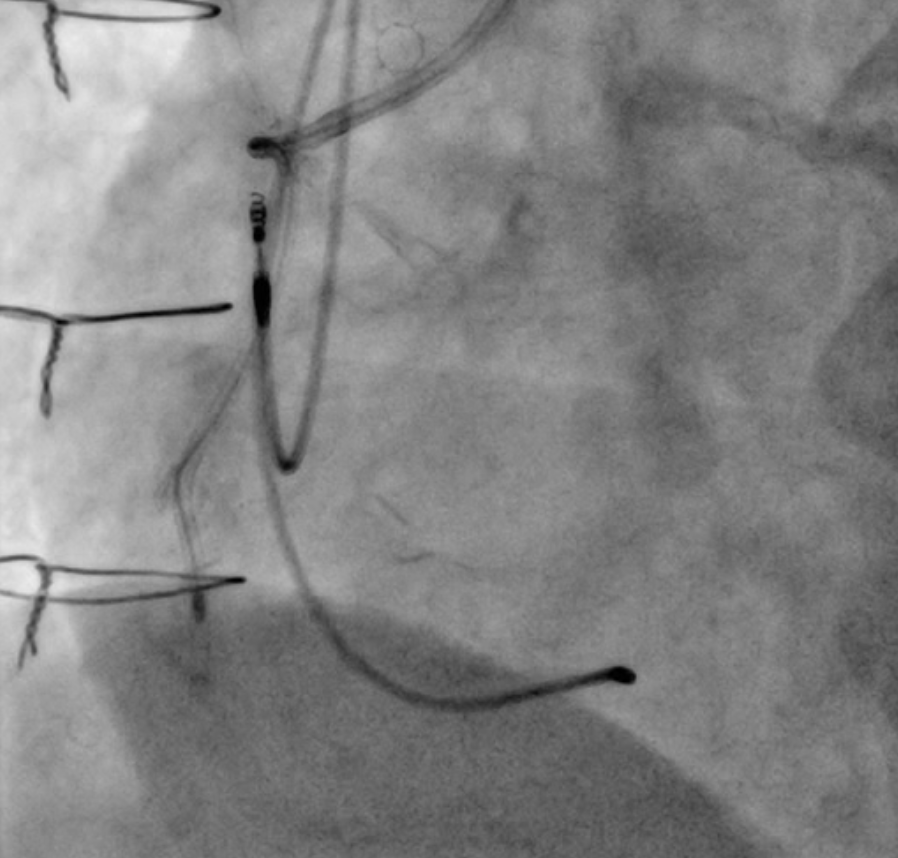
The cause of chest pain was suspected to be due to a lesion in the distal part of the RCA. We devised two strategies for approaching this distal lesion. One approach was to open the CTO lesion at the ostium of the RCA and then open the distal lesion. The other approach was to approach the distal lesion through SVG. Because of the strong calcification of the distal lesion, it was considered necessary to deliver a rotational atherectomy device(RA), and there was concern that approaching from the ostium of the RCA could carry a risk of complications such as cerebral embolism during using RA due to the severe calcification at the CTO. Therefore, it was believed to be relatively safer to perform rota via SVG, and the procedure was carried out.

Case Summary
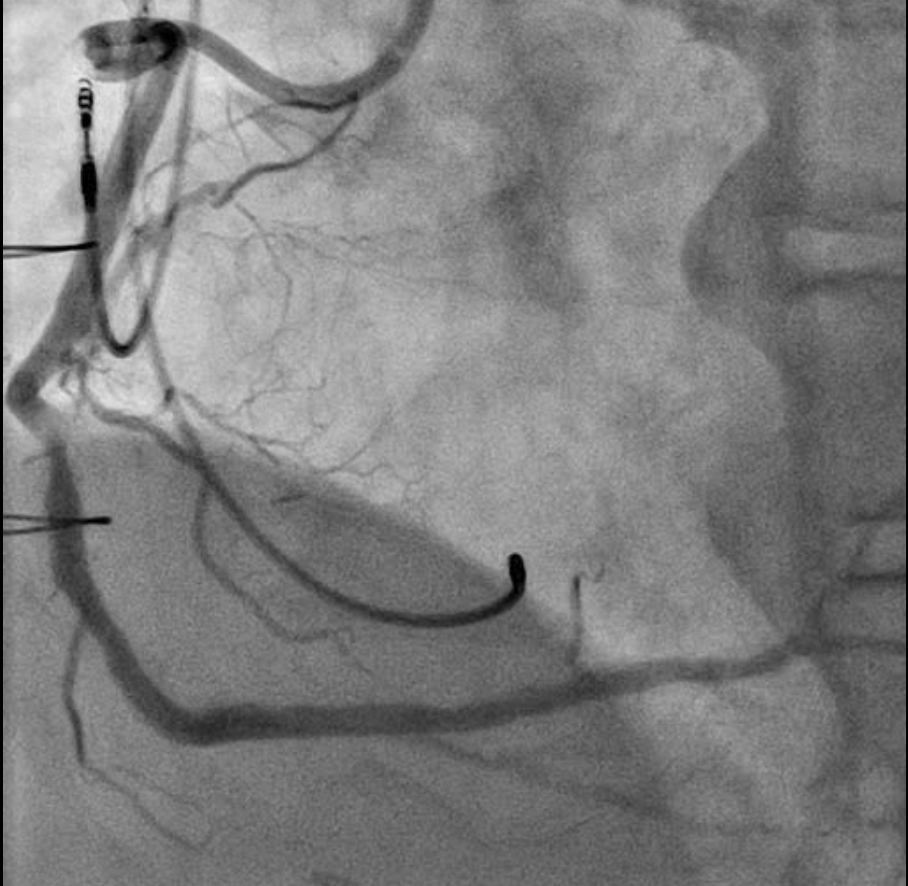
This case was a unique one where a bypass was performed to the mid RCA. In cases where a bypass is anastomosed to the distal RCA, the approach employed in this case may not have been possible because of the long length of SVG and difference in vessel diameter between SVG and RCA. So it was considered a rare case that RA could be performed due to SVG being shorter than conventional. We could deliver RA to the distal lesion safely, using a guide extension catheter.We experienced a case using RA via the bypass graft.