
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-192
Bail Out of an Inflated Renal Stent, Which Was Dislodged After Successful Deployment
By Dileep Kumar Tiwari, Amjad Ali
Presenter
Dileep Kumar Tiwari
Authors
Dileep Kumar Tiwari1, Amjad Ali2
Affiliation
Baderiya Metroprime Hospital, India1, Sagar Multispeciality Hospital, India2,
View Study Report
TCTAP C-192
Endovascular - Other Endovascular Intervention
Bail Out of an Inflated Renal Stent, Which Was Dislodged After Successful Deployment
Dileep Kumar Tiwari1, Amjad Ali2
Baderiya Metroprime Hospital, India1, Sagar Multispeciality Hospital, India2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
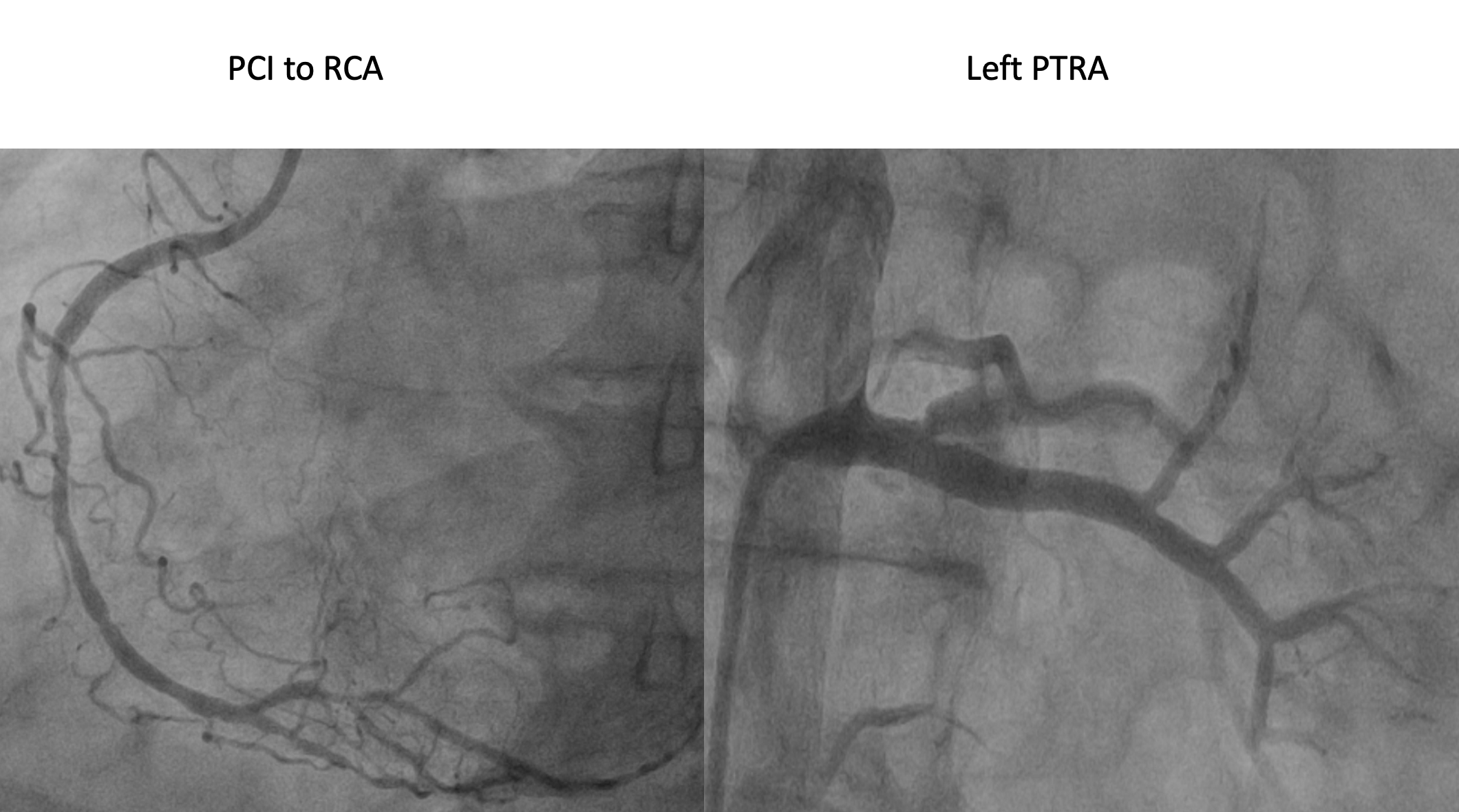
A 68-year-old gentleman who had a history of long-standing HTN, DM, and CKD (baseline creatinine 1.7 mg/dL) was presented with accelerated HTN, evolved IWMI, and acute LVF. His initial BP was 220/130 mmHg. After stabilization, he underwent coronary and renal angiography, which suggested TVD and bilateral critical renal artery stenosis. RCA was the infarct-related artery. Hence, PCI to RCA and, two days later, left PTRA was performed. One month later, he was readmitted for staged right PTRA.

Relevant Test Results Prior to Catheterization
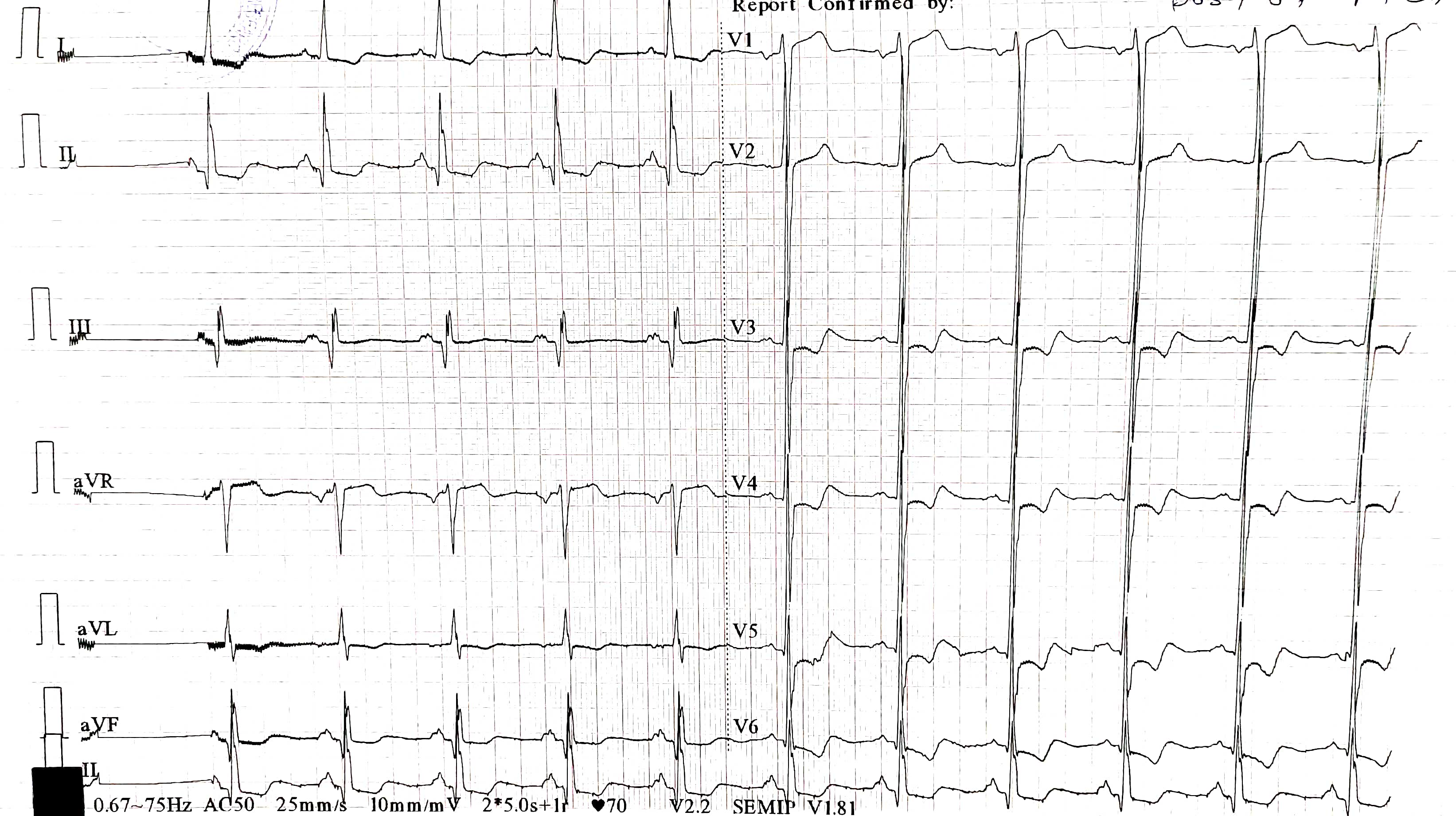
The patient remained stable after an index PCI to RCA and left PTRA. During this admission for staged right PTRA, his pulse rate was 88 bpm, BP was 134/82 mmHg, S. creatinine was 1.61 mg/dL, and random blood sugar was 175 mg/dL. His ECG showed LVH with LV strain pattern and Q waves in lead II, III, and aVF. The echocardiogram showed concentric left ventricular hypertrophy, no regional wall motion abnormalities, and LVEF was 60%.
Relevant Catheterization Findings
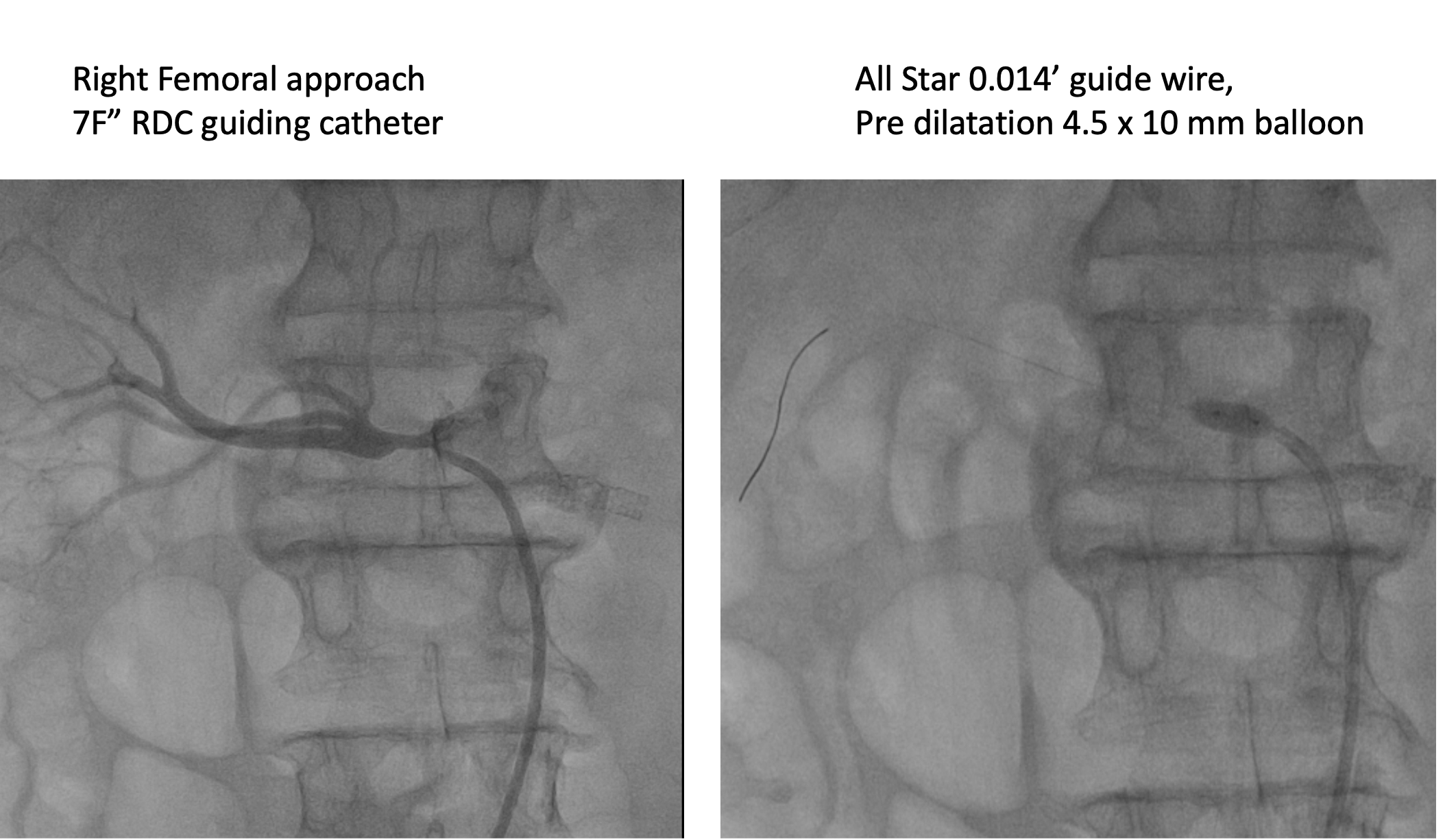
During the right PTRA, a renal artery was hooked with a 7 F' RDC guiding catheter and crossed with an all-star, 0.014 guide wire. The lesion was pre-dilated with a 4.5 x 10 mm NC balloon at 16 atm. Then, a 7 x 16 mm. Cogent BMS (Meril life sciences) stent was deployed at nominal pressure and post-dilated with the same balloon at 14 atm. The procedure went well. After removing the guide wire, the distal end of the stent shrunk, pushed back into the aorta, and finally dislodged in an inflated form.


Interventional Management
Procedural Step
We immediately rewired through the dislodging stent to stabilize between the aorta and renal artery. Left femoral access was taken and then upgraded to the 14 F" long sheath. Keeping the stent in position with the help of an RDC guiding catheter and all-star guide wire, first, we tried to pick the stent up with the bioptome, but the grasping strength was not enough to pull the stent inside the sheath. But in this process, the stent was dislodged from the guide wire and migrated down to the aortic bifurcation. The stent was jumping at the carina with each beat of the heart. At this moment, keeping the RDC catheter and long sheath at the level of the carina, we took a 20 mm snare system, and with lots of effort, we were able to pick the sten with snare and pull it down inside the sheath and finally take it out. Hence, the dislodged inflated renal stent was retrieved successfully without causing significant vascular injury. The long sheath was removed surgically. Two days later, the right PTRA was done successfully using a 7 x 16 mm Hippocampus (Medtronics) renal stent. Post-procedure, the patient was discharged from the hospital after 96 hours in stable condition.



Case Summary
Complications are part and parcel of the interventions, but dislodgement of an inflated stent after successful deployment is very rare. We should be prepared for unexpected complications during or after the interventions. Successful retrieval without much harm to the patient should be the goal of any bailout procedure. Appropriate thought processes and effective execution is the key to success.