
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-093
“Break the Calcium Rock” - A Challenging Case of Calcified Left Main Bifurcation Lesion With Rotashock and Impella Support in an Elderly Patient
By Yin Kei Jake Yeung, Alan Chan, Michael Kang-Yin Lee
Presenter
Yin Kei Jake Yeung
Authors
Yin Kei Jake Yeung1, Alan Chan1, Michael Kang-Yin Lee1
Affiliation
Queen Elizabeth Hospital, Hong Kong, China1,
View Study Report
TCTAP C-093
Coronary - Complex PCI - Left main
“Break the Calcium Rock” - A Challenging Case of Calcified Left Main Bifurcation Lesion With Rotashock and Impella Support in an Elderly Patient
Yin Kei Jake Yeung1, Alan Chan1, Michael Kang-Yin Lee1
Queen Elizabeth Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
An 84-year-old woman with a medical history of hypertension, hyperlipidemia, and ischemic heart disease with prior PCI done in 2015 was admitted to a private hospital for acute coronary syndrome. She presented mainly as persistent chest pain and shortness of breath on exertion. Physical examination revealed bilateral basal fine inspiratory crepitations with minimal pedal edema. Auscultation showed dual heart sounds without murmurs.

Relevant Test Results Prior to Catheterization
Chest X-Ray showed mild pulmonary congestion with bilateral upper lobe diversion. High-sensitive troponin I was 344 ng/L, and NT-proBNP was 642 ng/L. ECG showed sinus rhythm with no signs of ischemic changes. Echocardiography revealed an ejection fraction of 45% with mild mitral regurgitation.
Relevant Catheterization Findings
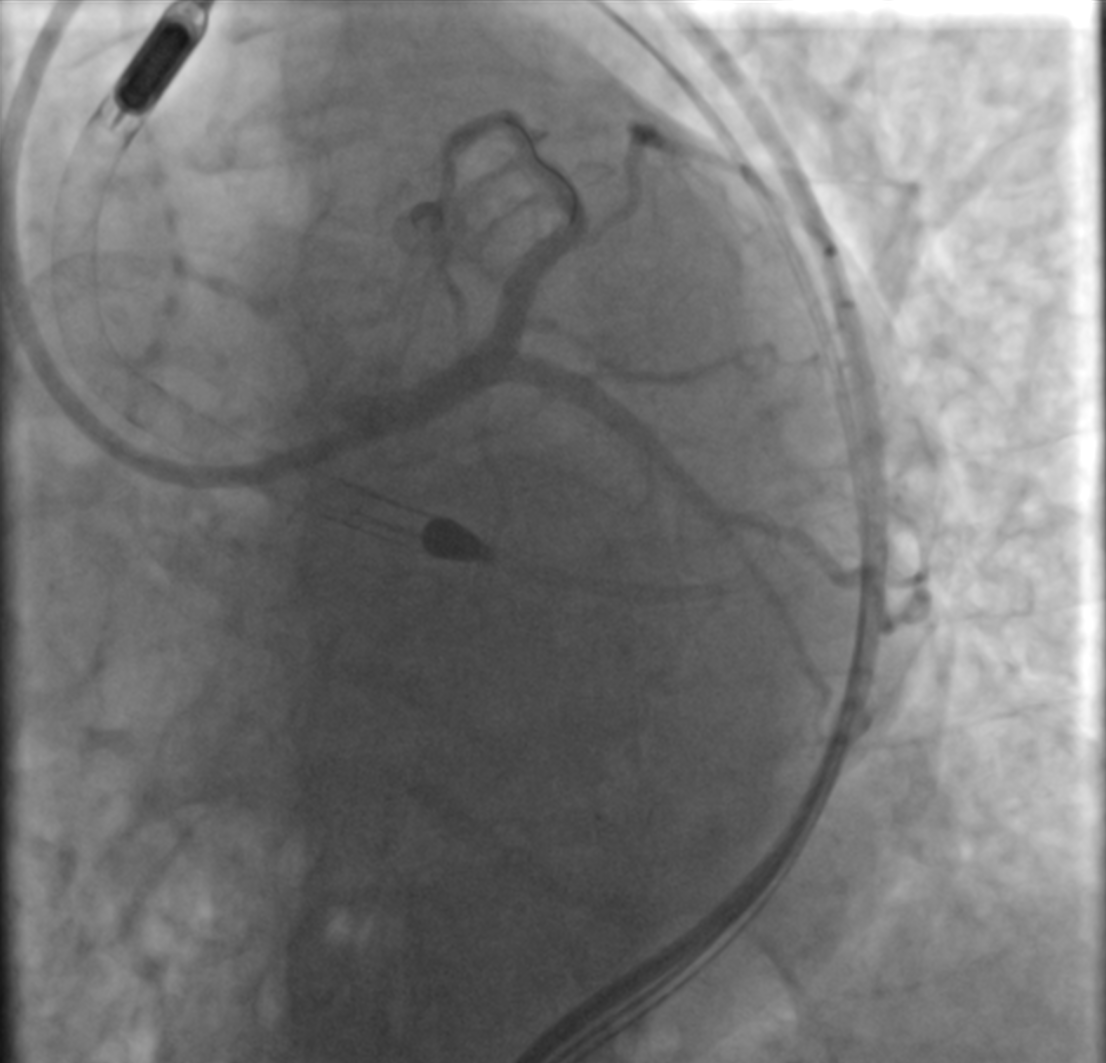
Coronary angiography was performed at the private hospitalLeft Main (LM): Severe distal LM disease with protruding calcium, Medina classification 1,1,1LAD: Severe ostial-proximal calcified disease, mid LAD stent patentLCx: Severe ostial subtotal occlusion, proximal LCx stent patentRCA: Severe stenosis over proximal-mid RCAShe was referred to our hospital for revascularization, and after discussions with the Heart team, she opted for impella-assisted high-risk PCI instead of CABG.



Interventional Management
Procedural Step
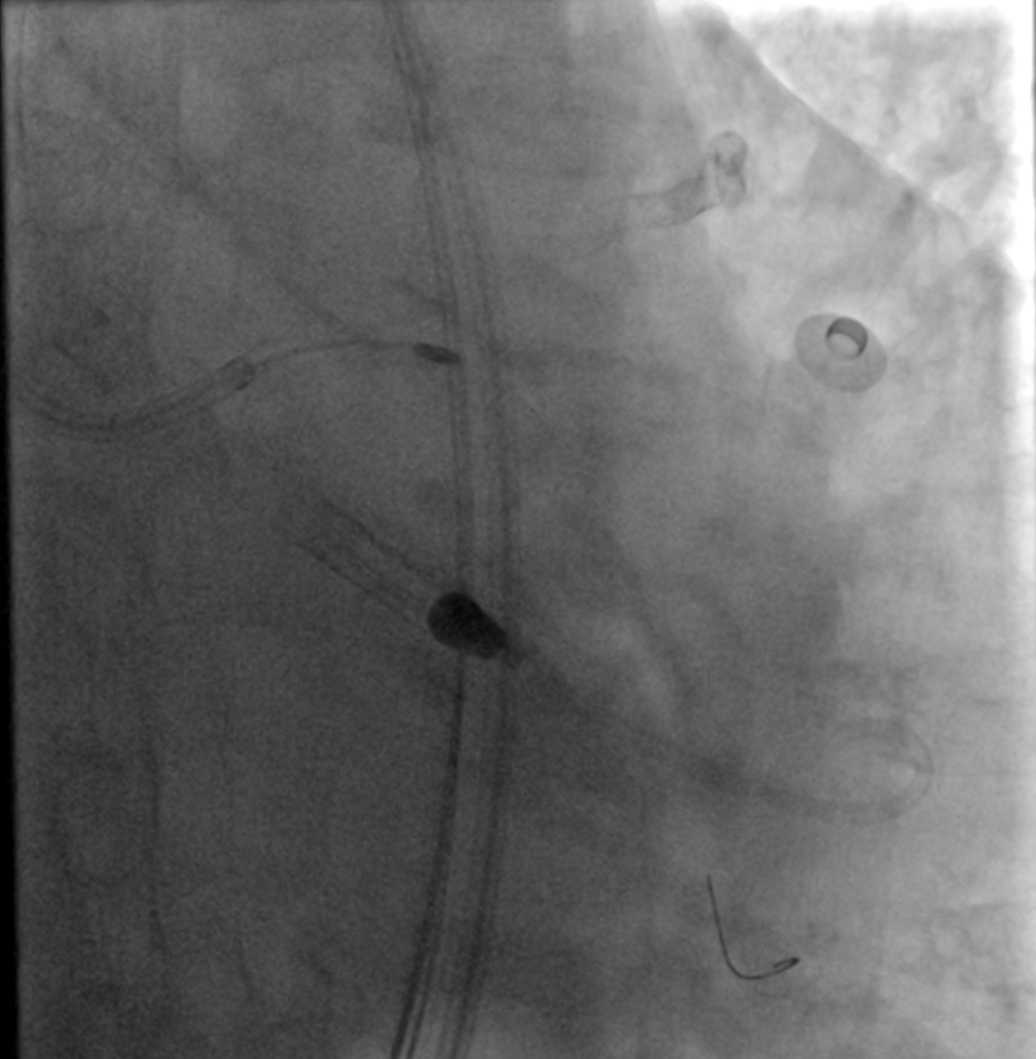
The Impella CP device was inserted via the right femoral artery using a single-access technique and a 7 Fr Destination sheath through the impella sheath. PCI was initially performed on the RCA, with two overlapping stents placed in the proximal-mid RCA. Subsequently, PCI was performed on the left coronary artery.Despite attempting various techniques and wires, wiring the LCx proved challenging due to angulation and hard protruding calcium. Rotablation was used for plaque modification in the distal-LM and proximal LAD, but LCx wiring remained unsuccessful with the use of dual-lumen catheters, reverse wire technique, and different wires such as Sion Black wire and Fielder XT-R wire. Eventually, successful wiring of the LCx was achieved by penetrating through the calcified lesion using a Gaia Next 2 wire. Rotablation was then performed on the LM-proximal LCx using a Rotapro 1.5 burr.Following predilatation of LM-LAD and LM-LCx with NC balloons, intravascular lithotripsy was employed to further prepare the lesions. Subsequent intravascular ultrasound (IVUS) confirmed adequate lesion preparation with significant calcium cracking. The LM bifurcation lesion was stented using the DK-Crush stenting strategy.Post-PCI, the Impella CP device was removed, and the right femoral wound was closed using a Proglide and an 8 Fr Angioseal.

Case Summary
The case of an elderly patient with a complex left main bifurcation lesion featuring severe calcifications highlights the challenges associated with advanced coronary artery disease. This case demonstrates the successful utilization of various endovascular devices, equipment, and techniques to tackle this highly intricate condition.