
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-075
An Attack on Both Fronts: An Angulated Chronic Total Occlusion Requiring Simultaneous Antegrade Real Time IVUS-Guided Puncture and Reverse CART Technique
By Jeffrey Chun-Yin Lee, Frankie CC Tam
Presenter
Jeffrey Chun-Yin Lee
Authors
Jeffrey Chun-Yin Lee1, Frankie CC Tam2
Affiliation
Grantham Hospital, Hong Kong, China1, Queen Mary Hospital, Hong Kong, China2,
View Study Report
TCTAP C-075
Coronary - Complex PCI - CTO
An Attack on Both Fronts: An Angulated Chronic Total Occlusion Requiring Simultaneous Antegrade Real Time IVUS-Guided Puncture and Reverse CART Technique
Jeffrey Chun-Yin Lee1, Frankie CC Tam2
Grantham Hospital, Hong Kong, China1, Queen Mary Hospital, Hong Kong, China2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
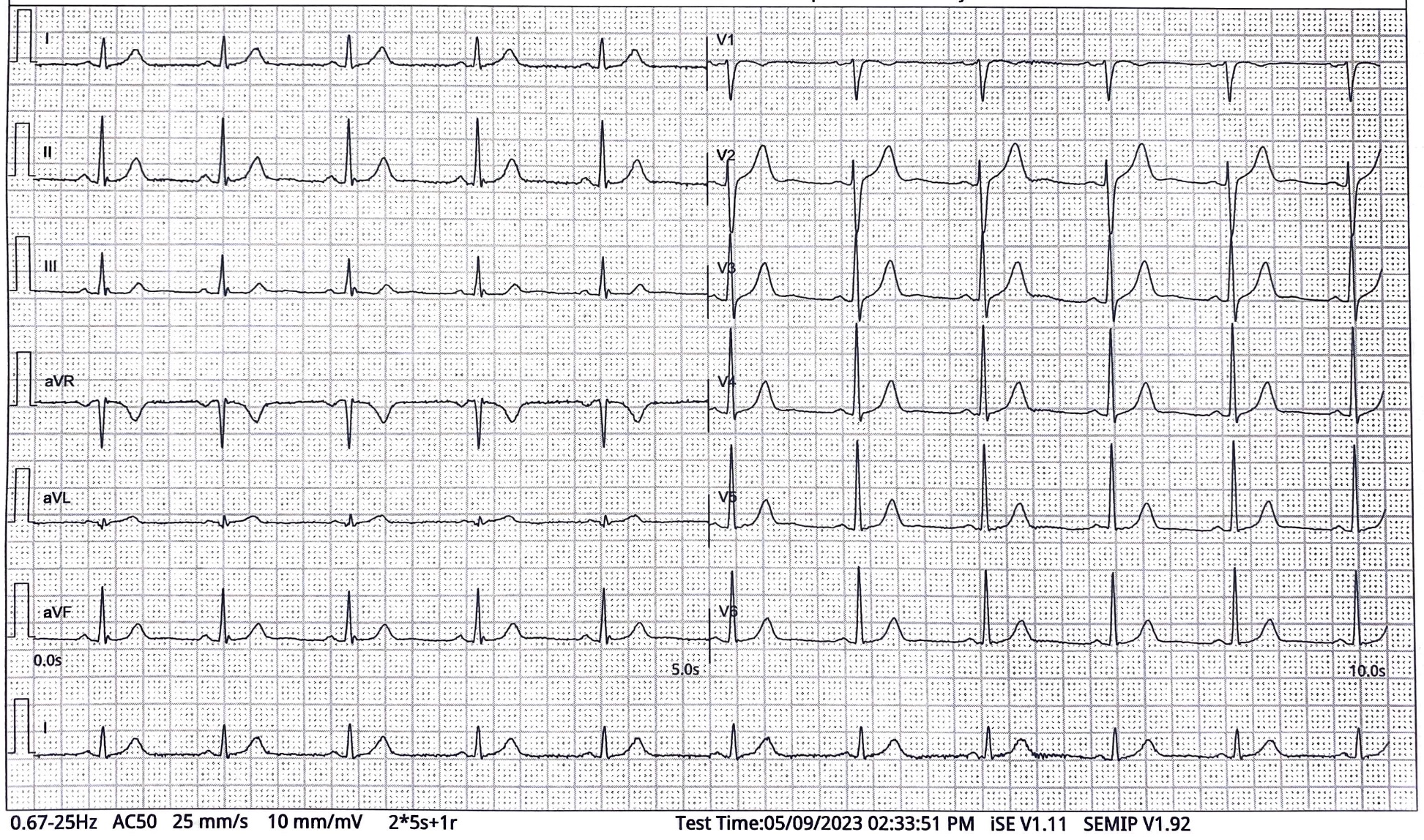
Our patient is a 49 years old man, with a history of untreated hyperlipidaemia and chronic smoking. He was admitted to our hospital for progressively worsening chest pain. On admission, his vital signs and physical examination were unremarkable. ECG did not show any ST changes. High sensitivity troponin was elevated at 300 ng/L (cutoff <100 ng/L). Echocardiogram showed a normal ejection fraction with no regional wall abnormalities. A diagnosis of NSTEMI was made.

Relevant Test Results Prior to Catheterization
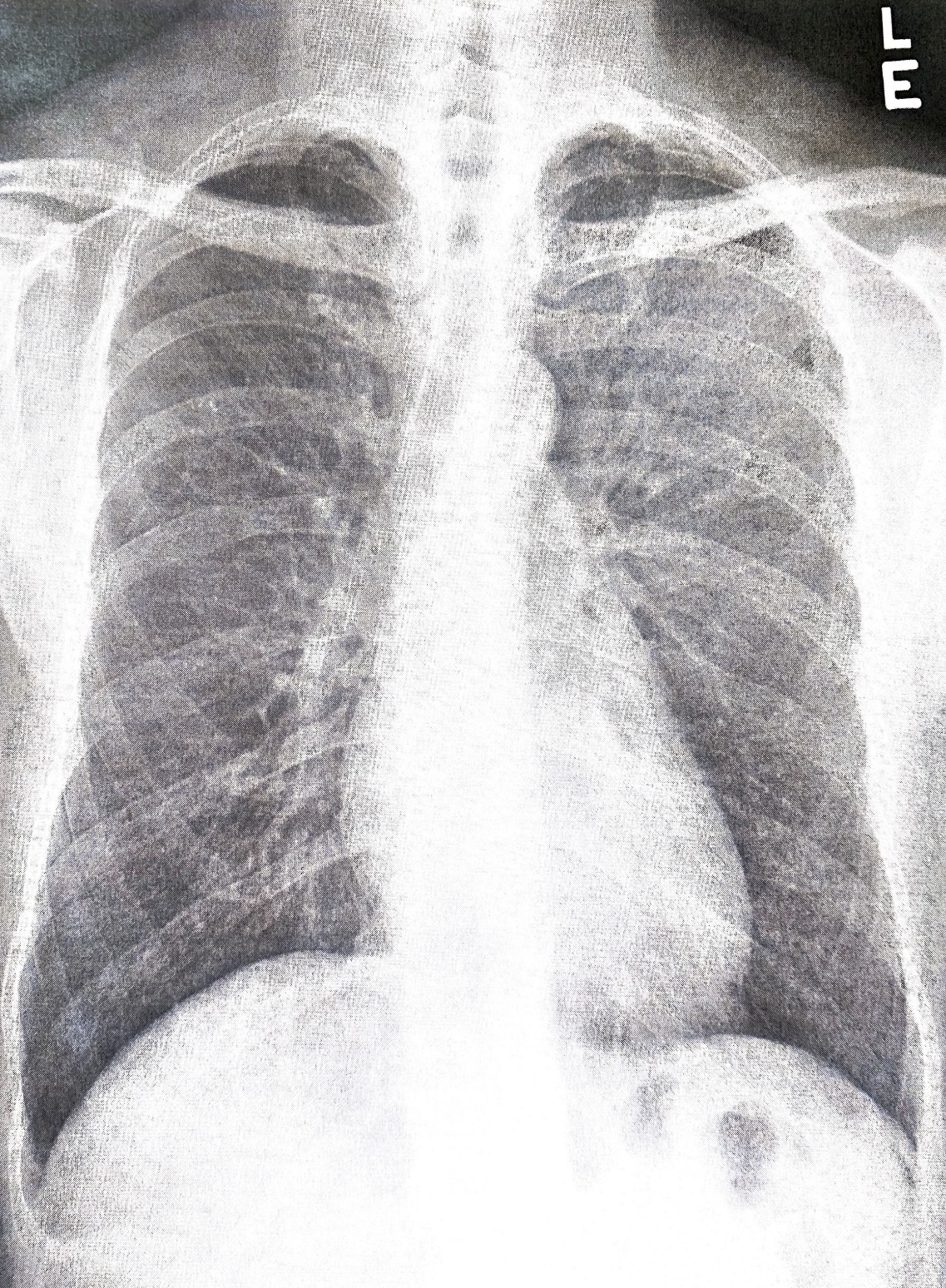
Investigations for the patient were done. As described, the high sensitivity troponin was elevated at 300 ng/L. ECG and Echo were grossly unremarkable. Chest X-ray was also clear of congestion. His total cholesterol was 5.8 mmol/L and low-density lipoprotein was 3.8 mmol/L; which were both increased. His baseline complete blood count, kidney and liver function tests were unremarkable.
Relevant Catheterization Findings
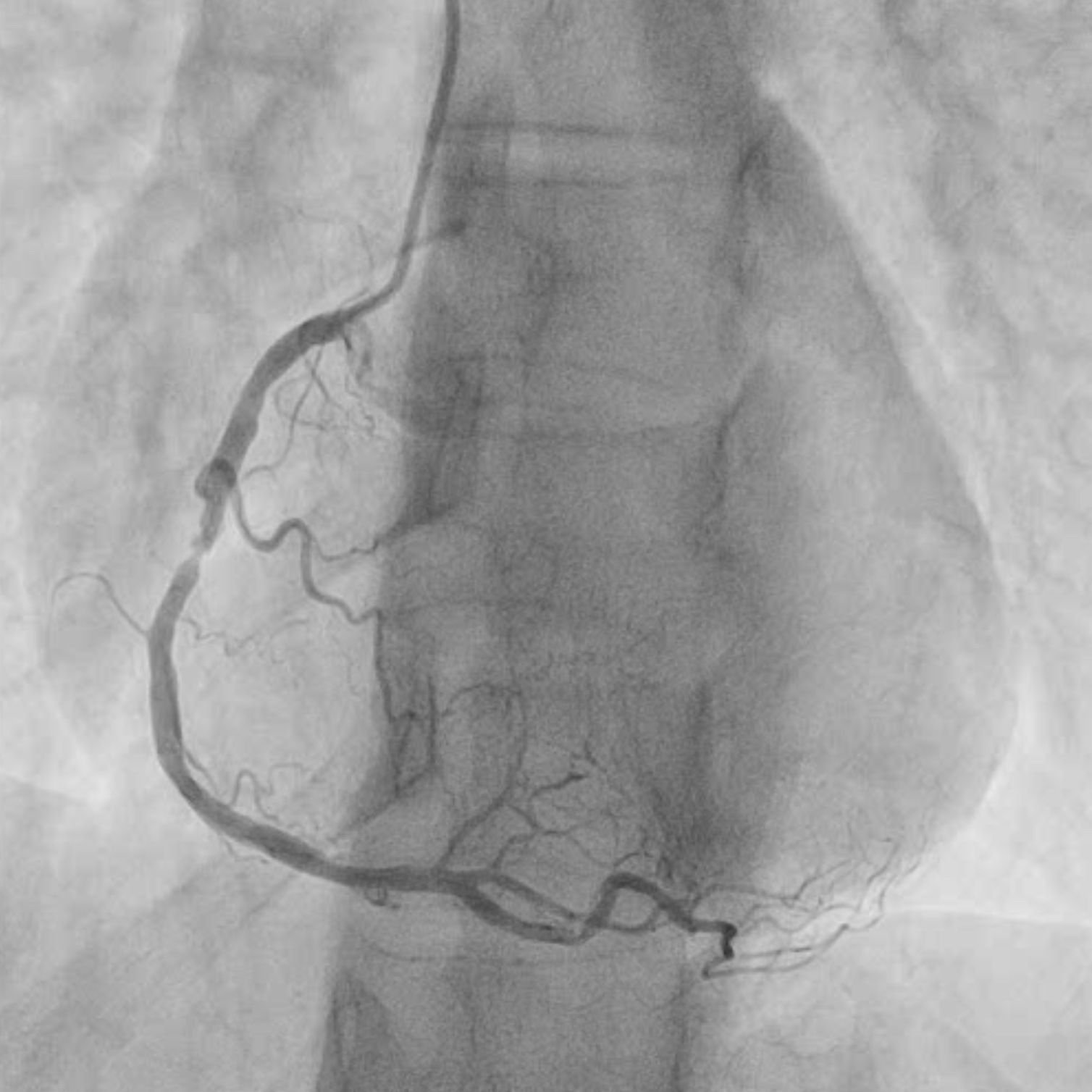
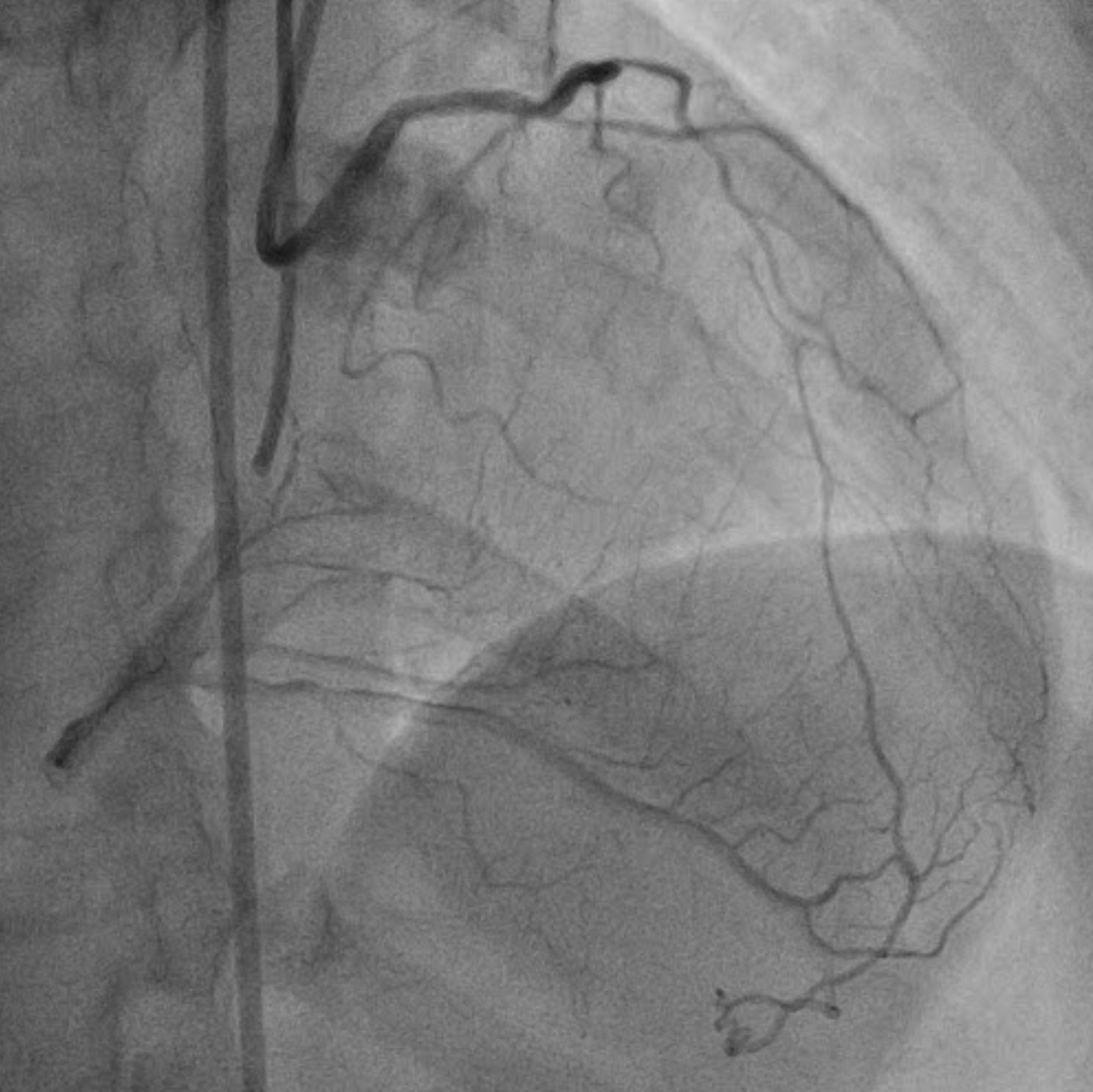
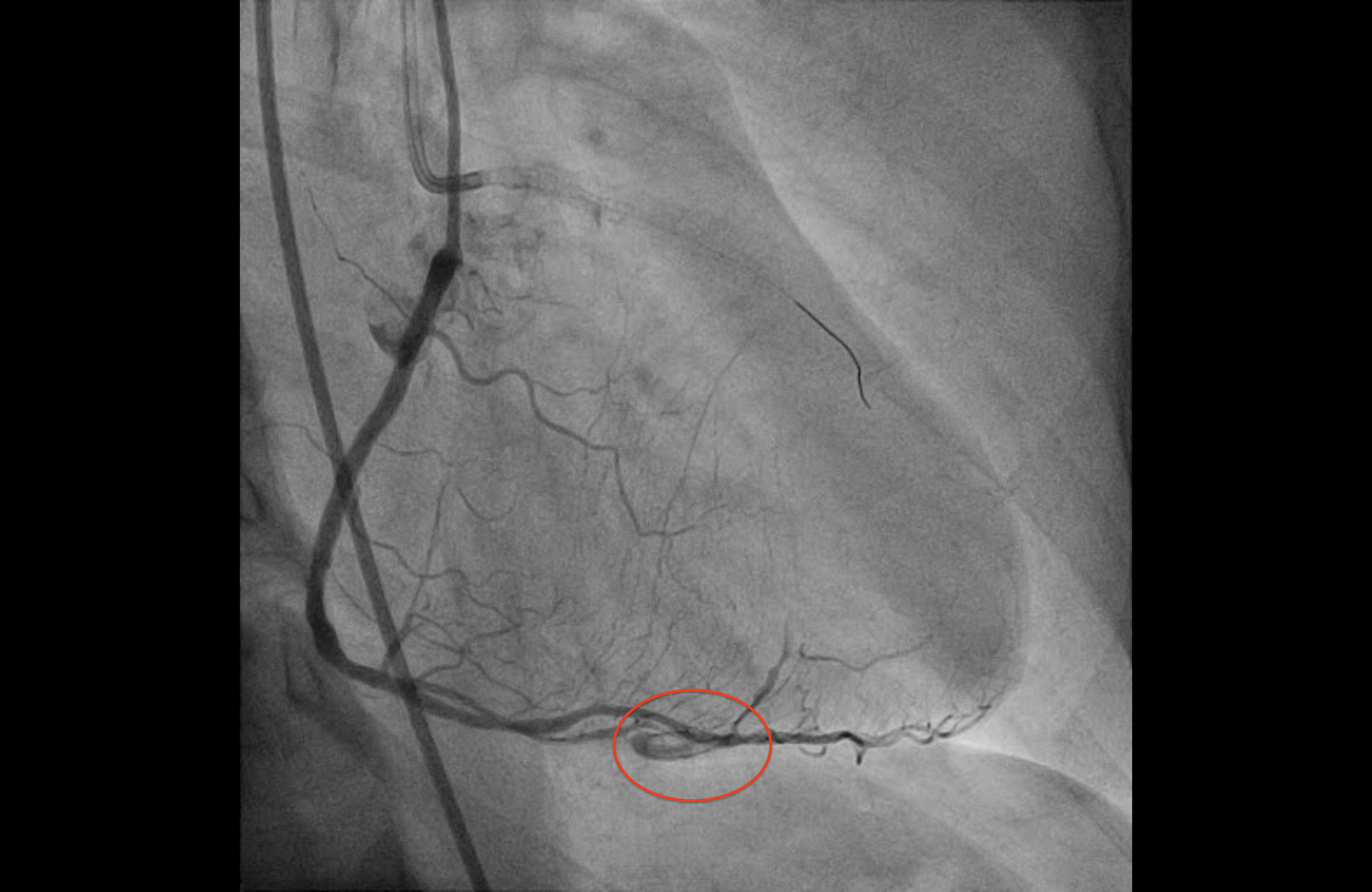
Coronary angiogram showed a mid-RCA 99 % focal stenosis, to which PCI was done. There was also an ostial LAD CTO, with right to left collaterals.
The patient declined CABG, and underwent staged PCI to LAD CTO. We attempted antegrade wiring first, but could not cross the CTO body. Retrograde wiring through a septal collateral (S2) was also difficult due to side branch angulation. Eventually the procedure was aborted. The patient was then brought back for a second CTO PCI attempt.

Interventional Management
Procedural Step
We obtained two vascular access for bilateral injection: 7 Fr EBU 3.5 (Medtronic) and 6 Fr IL 3.5 (Terumo) guide catheters were used. Repeat angiogram showed a long ostial LAD CTO with an ambiguous stump (J-CTO score 4). First, we wired the Ramus branch, and located the CTO proximal cap with IVUS (Terumo Navifocus). Real time IVUS guided puncture was done with a Conquest Pro 12 wire (Asahi). However, we failed to negotiate through the CTO body. Then, we switched to the retrograde approach. We successfully crossed our target septal collateral (S4) using a SUOH03 wire (Asahi). A Caravel microcatheter (Asahi) could not pass; eventually the septal collateral was dilated with a Turnpike LP microcatheter (Teleflex). Retrograde wiring with a Fielder XTA wire (Asahi) also could not negotiate through the CTO body into the left main true lumen (as confirmed by IVUS), despite many attempts. Hence, we decided to perform the REVERSE CART technique, which was successful. Subsequently, we performed wire externalisation, removed the retrograde equipment and switched back to an antegrade workhorse wire. PCI to the LAD was done under IVUS guidance, using a 3.5 mm x 19 mm and a 2.0 mm x32 mm Coroflex stent (B. Braun). The post-stenting angiogram showed contrast extravasation from the septal collateral, which was managed with protamine reversal. The patient remained haemodynamically stable, and the final angiogram showed no further staining with TIMI III flow.


Case Summary
This case illustrates how challenging CTOs can be, especially those with an ambiguous proximal cap and ending in a bifurcation distally. IVUS can be useful to resolve the proximal cap ambiguity and guide re-entry of the retrograde wire into the true lumen. The choice of interventional collaterals is important as well, especially if it is angulated from the CTO body. While dilating septal collaterals are generally safe, one must be aware of the choice of microcatheters and the occurrence of perforation. Lastly, one should not be afraid to utilise the subintimal space with dissection/re-entry techniques, when true lumen crossing is challenging.