
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-066
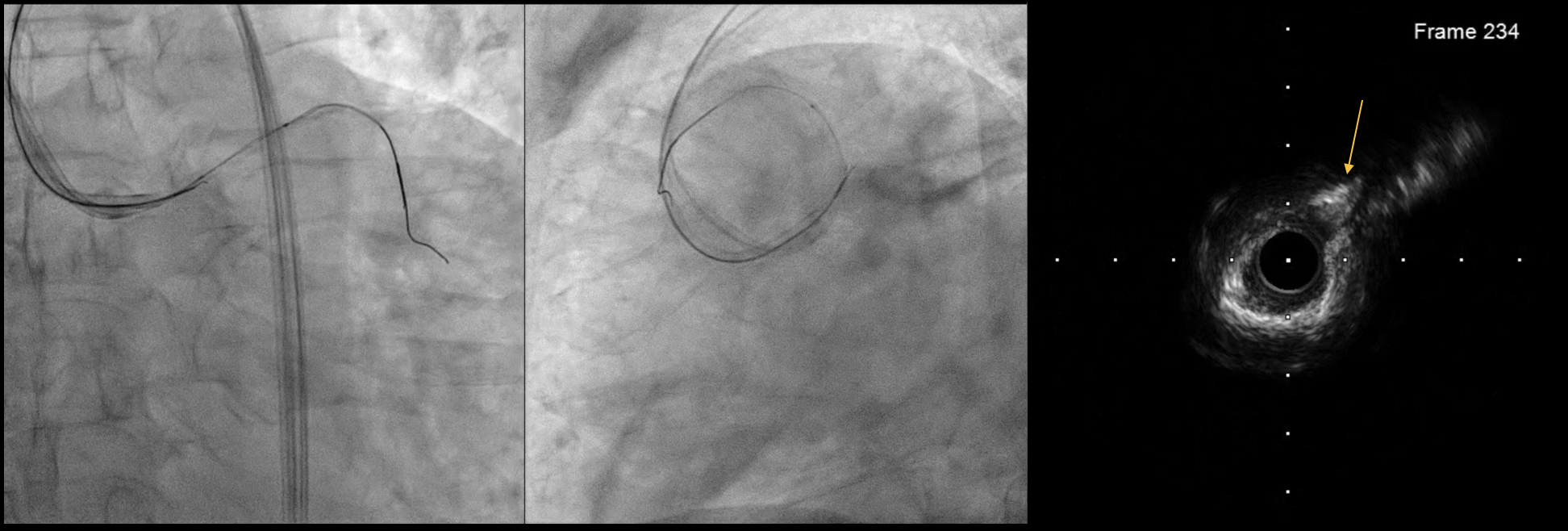
Intravascular Ultrasound-Guided Antegrade Approach for Left Main Coronary Artery Chronic Total Occlusion
By Jian Kuan Yeh, Cheng Yu Ko
Presenter
Jian Kuan Yeh
Authors
Jian Kuan Yeh1, Cheng Yu Ko1
Affiliation
National Cheng Kung University Hospital, Taiwan1,
View Study Report
TCTAP C-066
Coronary - Complex PCI - CTO
Intravascular Ultrasound-Guided Antegrade Approach for Left Main Coronary Artery Chronic Total Occlusion
Jian Kuan Yeh1, Cheng Yu Ko1
National Cheng Kung University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
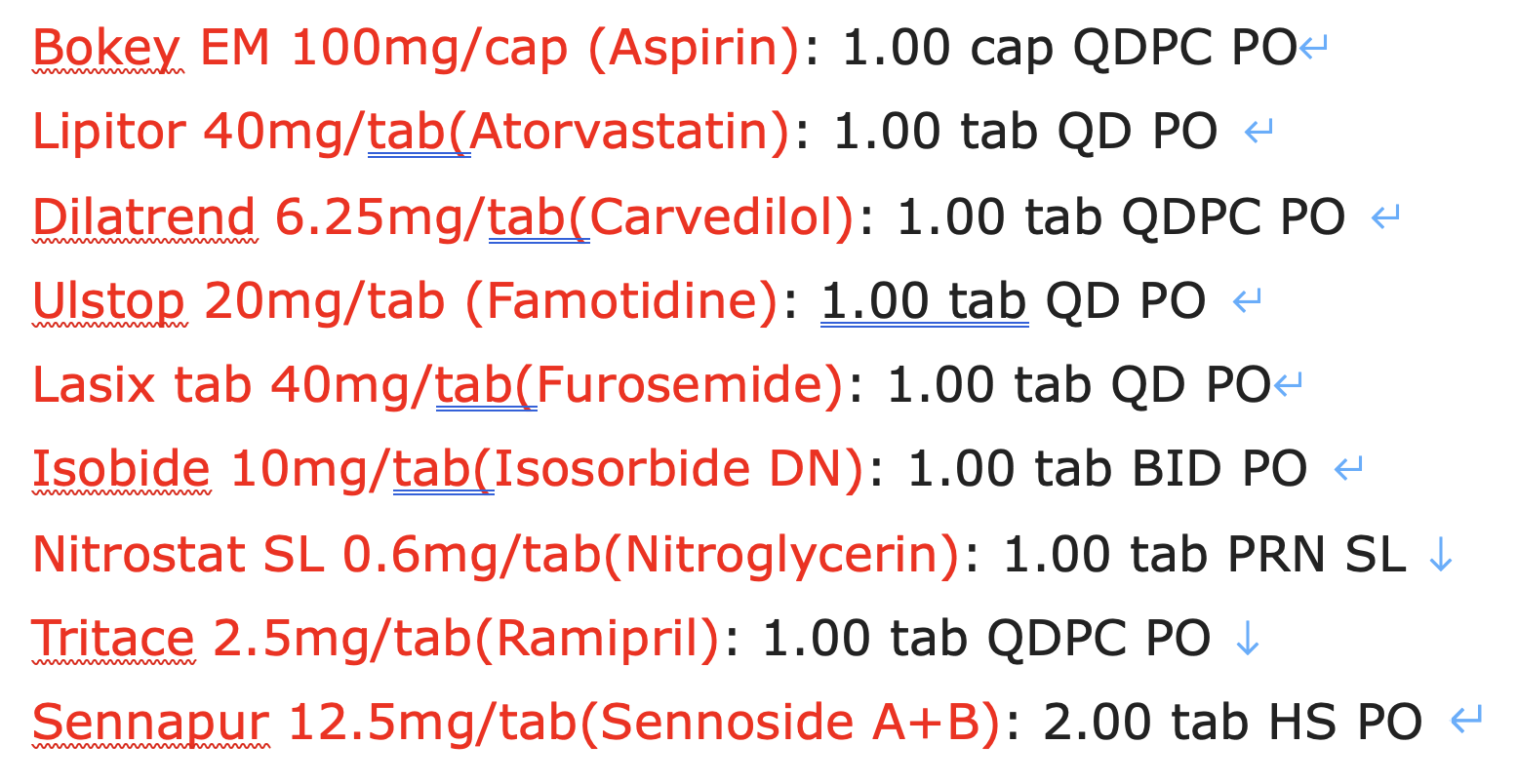
The patient is a 69-year-old male smoker with history of hyperlipidemia. He presented with retrosternal chest tightness aggravated by exercise and relieved by for 6 months. Physical examination results were unremarkable. He was started on anti-anginal medications, but his chest pain was refractory to medical treatment.
Relevant Test Results Prior to Catheterization
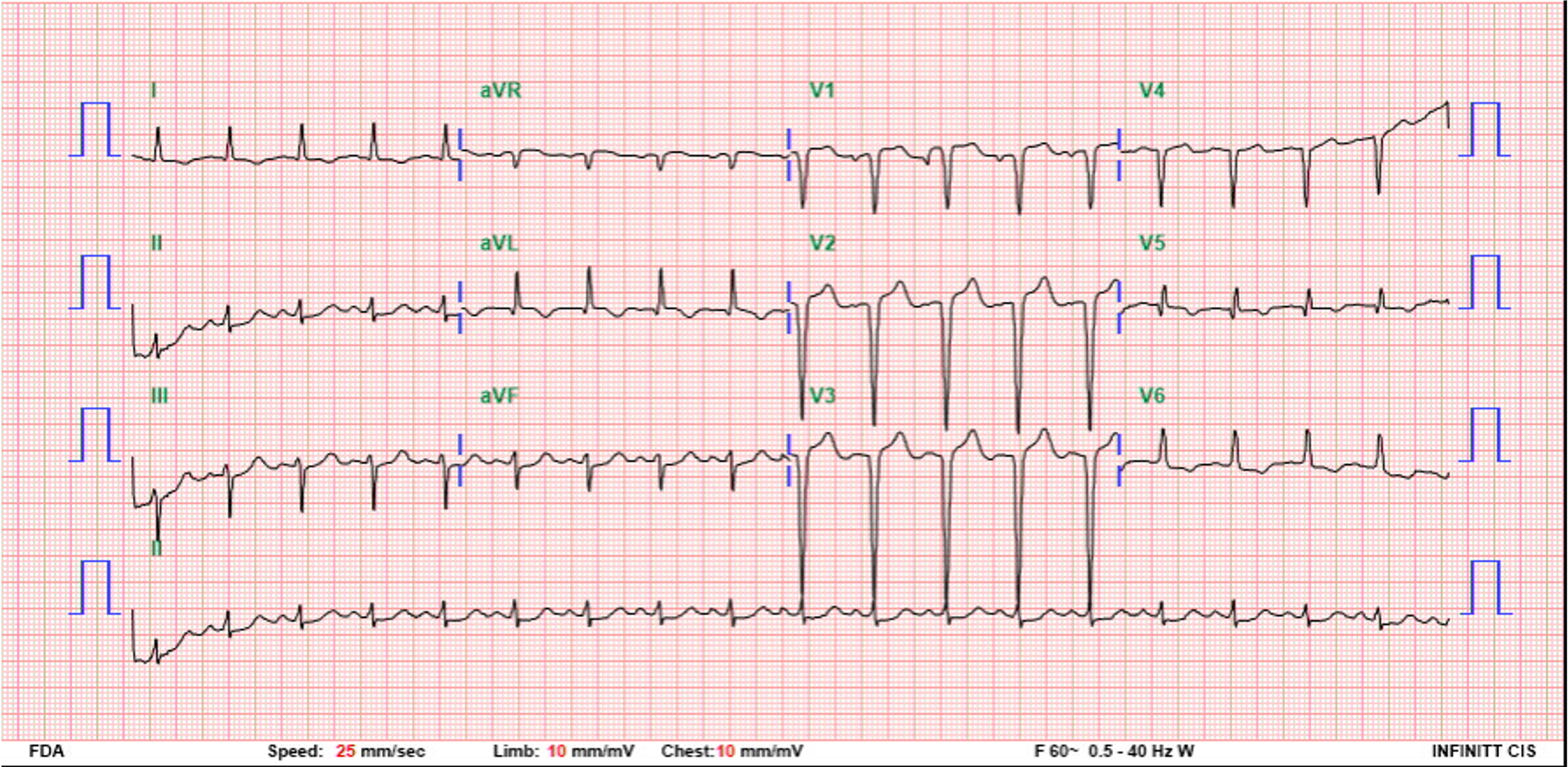
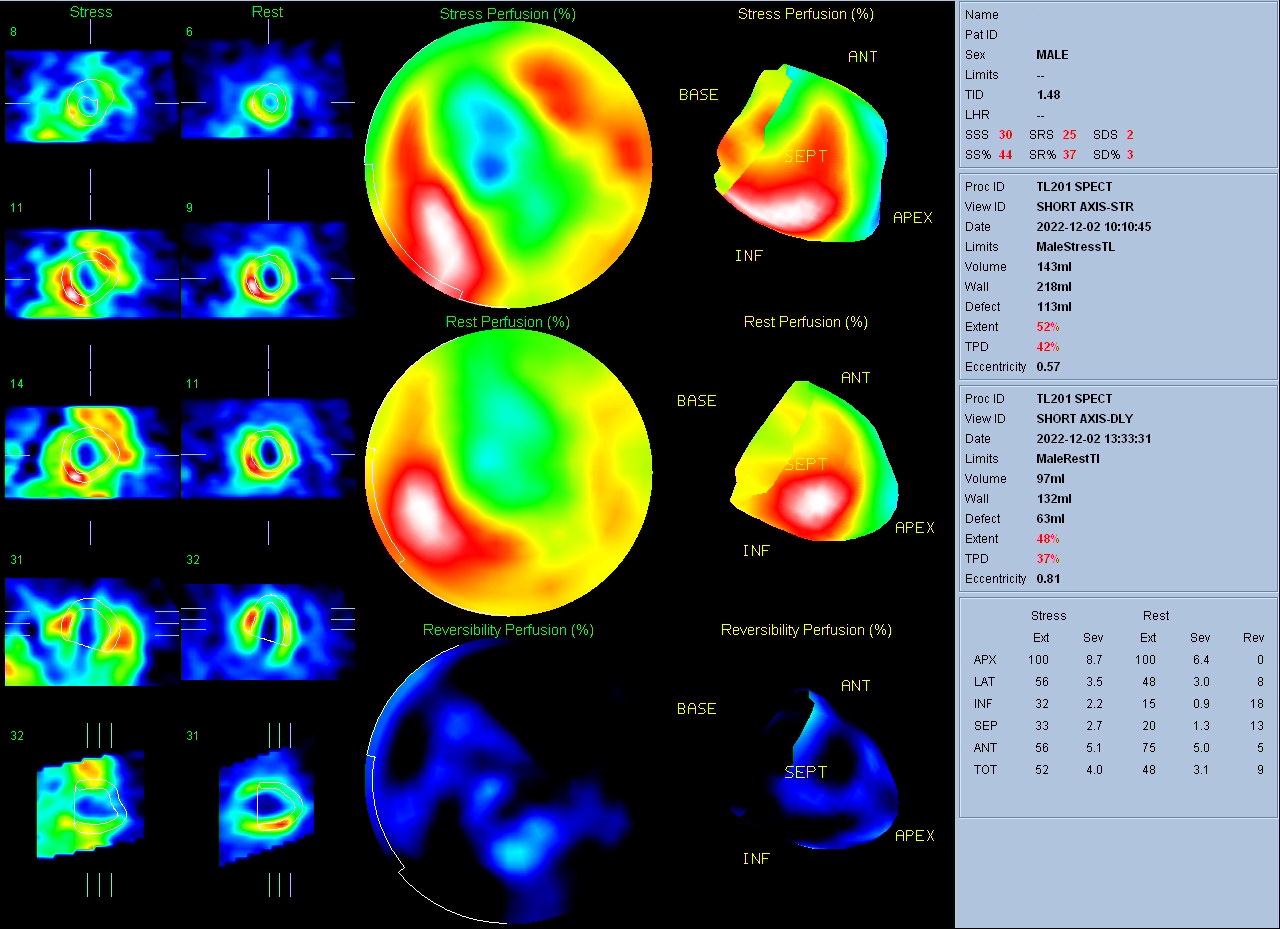
Electrocardiogram showed anterior Q waves. Trans-thoracic echocardiography showed impaired global left ventricular systolic function with an estimated ejection fraction of 34% by 2D along with regional wall motion abnormalities. Thallium myocardial perfusion scan showed large ischemia regions over anterior and anteroseptal regions.

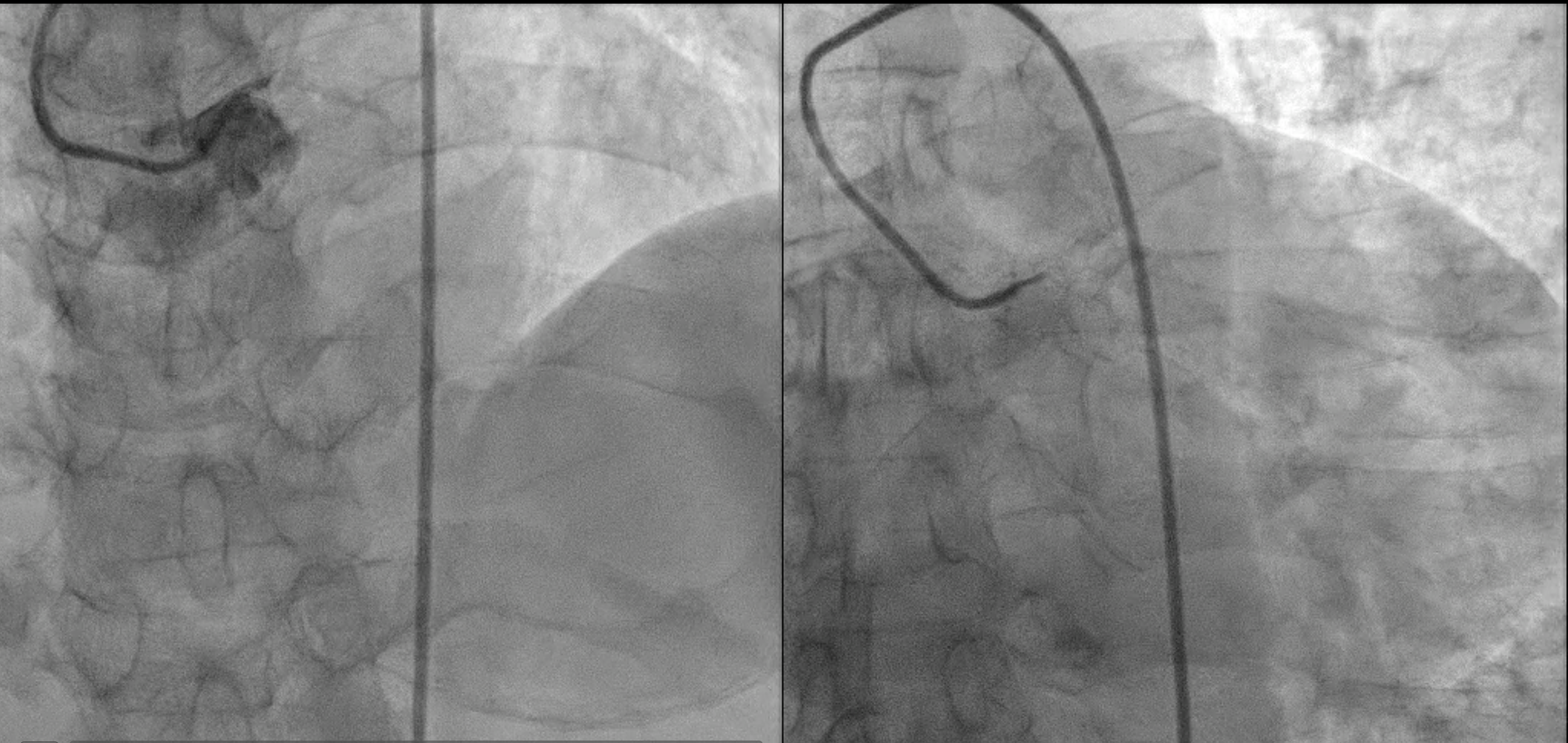
Relevant Catheterization Findings
Left Main: Atherosclerosis, total occlusion since dLMLAD: Atherosclerosis, total occlusion

Interventional Management
Procedural Step
1. An EBU 3.5 SH 7 Fr. guiding catheter to engage LM orifice.

Case Summary
1. Dual injection is imperative in selecting strategy to treat CTO and wire selection.2. When there is vague proximal cap, IVUS-guided puncture may be needed.3. The ping pong guide catheter technique may be utilized to facilitate real time IVUS-guided puncture.