
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-091
A Challenging Case Report of Complex Critical Left Main Bifurcation Percutaneous Coronary Intervention (PCI): Hualai River
By Wittawat Wattanasiriporn
Presenter
Wittawat Wattanasiriporn
Authors
Wittawat Wattanasiriporn1
Affiliation
Internal Medicine Department, Division of Cardiology, Rajavithi Hospital, College of Medicine, Rangsit University, Thailand1,
View Study Report
TCTAP C-091
Coronary - Complex PCI - Left main
A Challenging Case Report of Complex Critical Left Main Bifurcation Percutaneous Coronary Intervention (PCI): Hualai River
Wittawat Wattanasiriporn1
Internal Medicine Department, Division of Cardiology, Rajavithi Hospital, College of Medicine, Rangsit University, Thailand1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
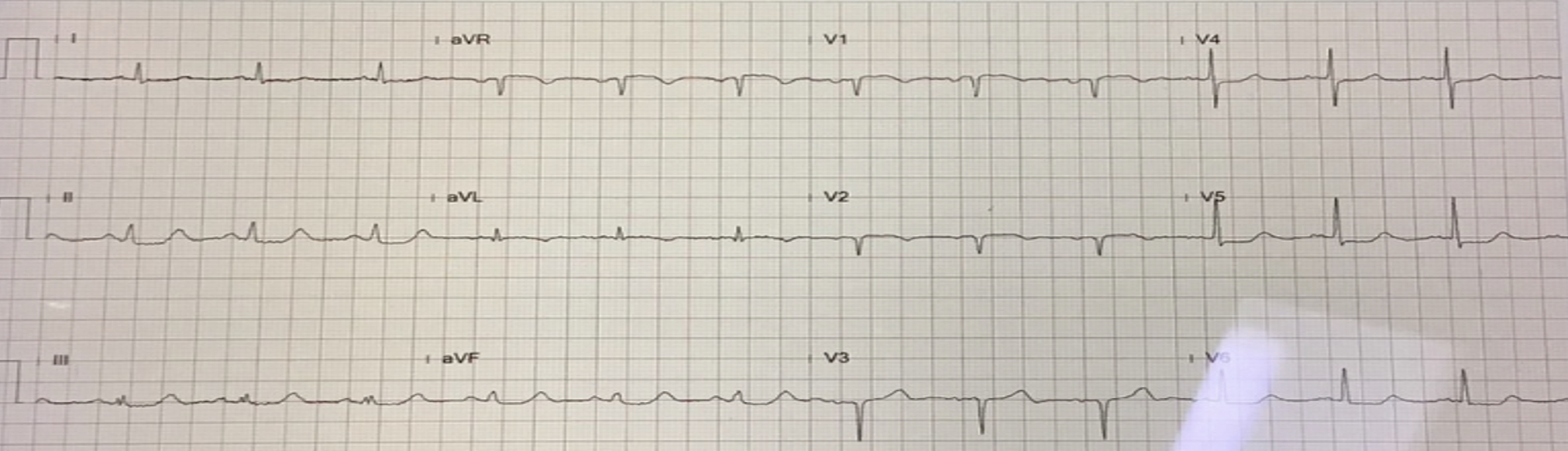
Thai female 77 years, risk HT, DLP presented with chest pain 8 hours prior to admission. BP 104/62 mmHg, HR 76 bpm, heart normal s1, s2, no murmur, Lungs clear. EKG showed Normal sinus rhythm, diffused depression c ST elevation at aVR. Echocardiogram showed LVEF 42%, Hypokinesia at anterior, anteroseptal, anterolateral wall, no significant valvular heart disease. Troponin T 30,000 pg/ml.
Relevant Test Results Prior to Catheterization
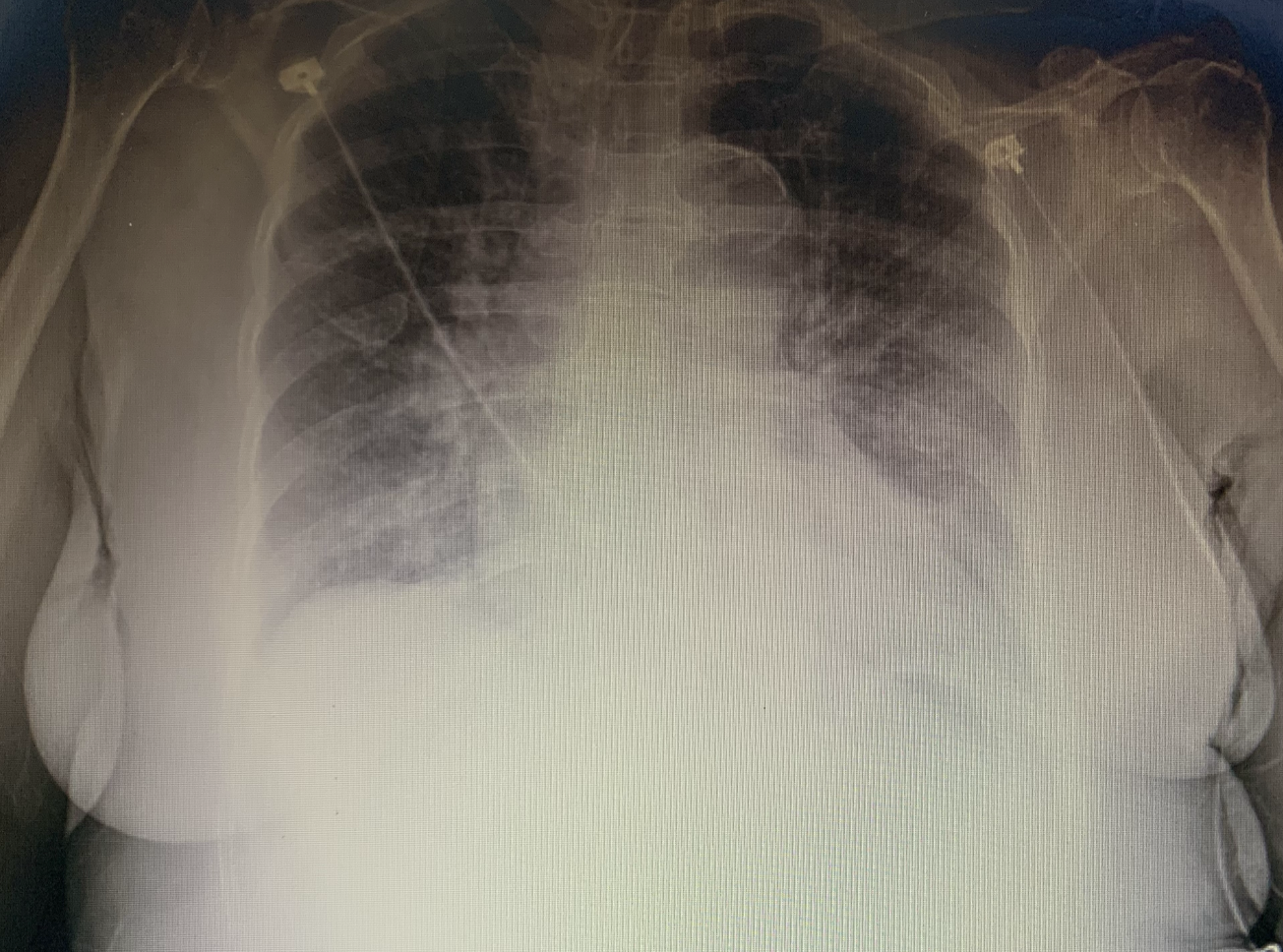
EKG showed Normal sinus rhythm, diffused depression c ST elevation at aVR.Echocardiogram showed LVEF 42%, Hypokinesia at anterior, anteroseptal, anterolateral wall, no significant valvular heart disease. Troponin T 30,000 pg/ml.CXR showed cardiomegaly c pulmonary congestion
Relevant Catheterization Findings
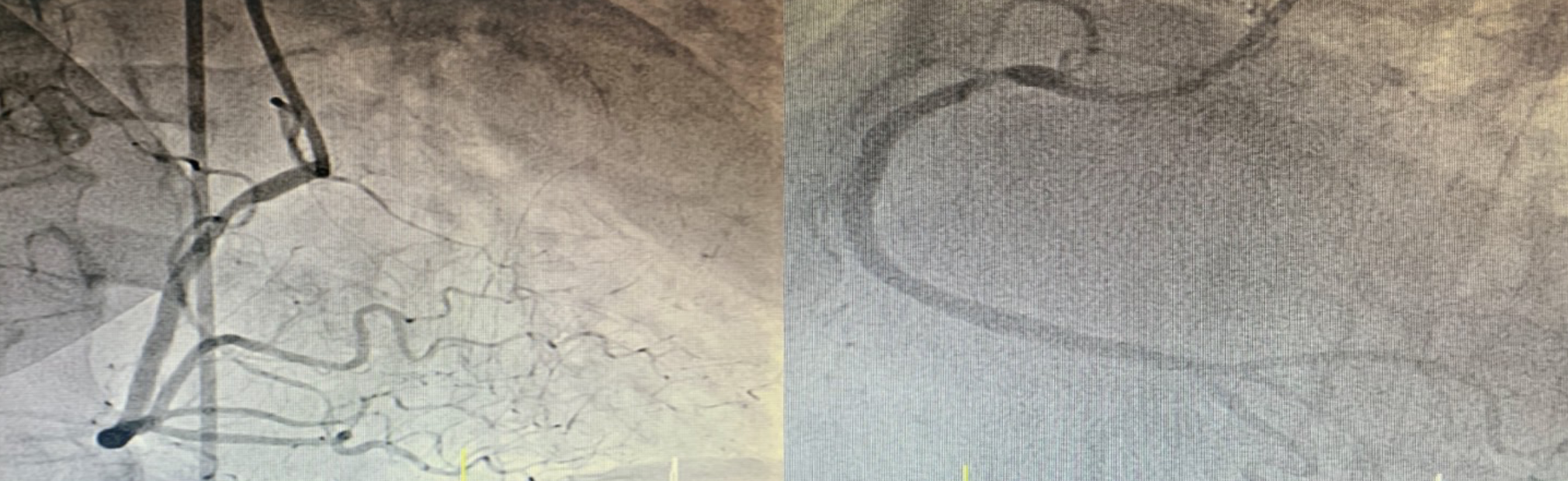
CAG via right femoral approach with JL 3.5/6 Fr, JR 3.5/6 Fr diagnostic catheterRt dominantLM: 95% stenosis ostial LMLAD: 70% stenosis proximal LADLCx: non significant stenosisRCA: 70% stenosis proximal RCA, give collateral to LCCA

Interventional Management
Procedural Step
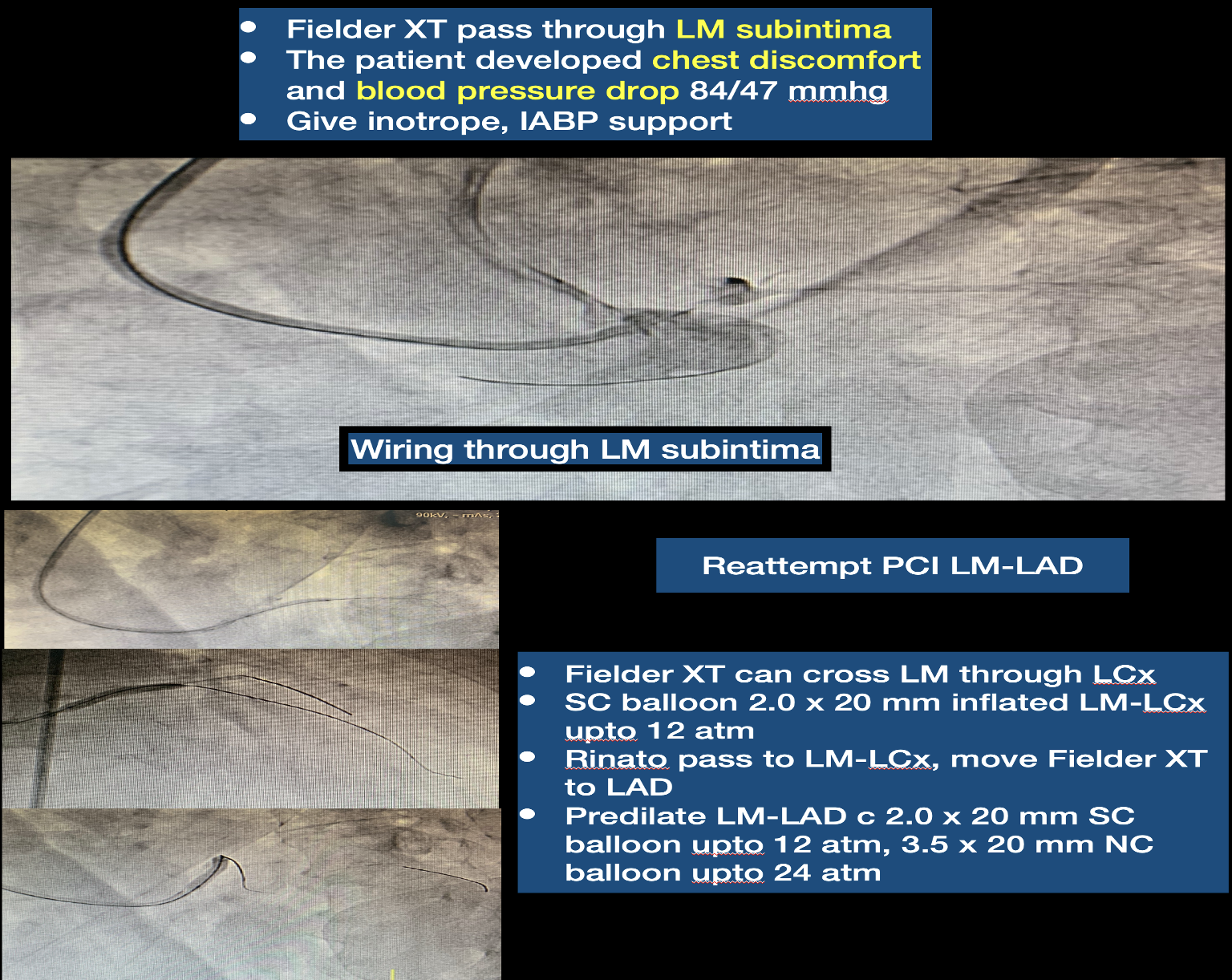
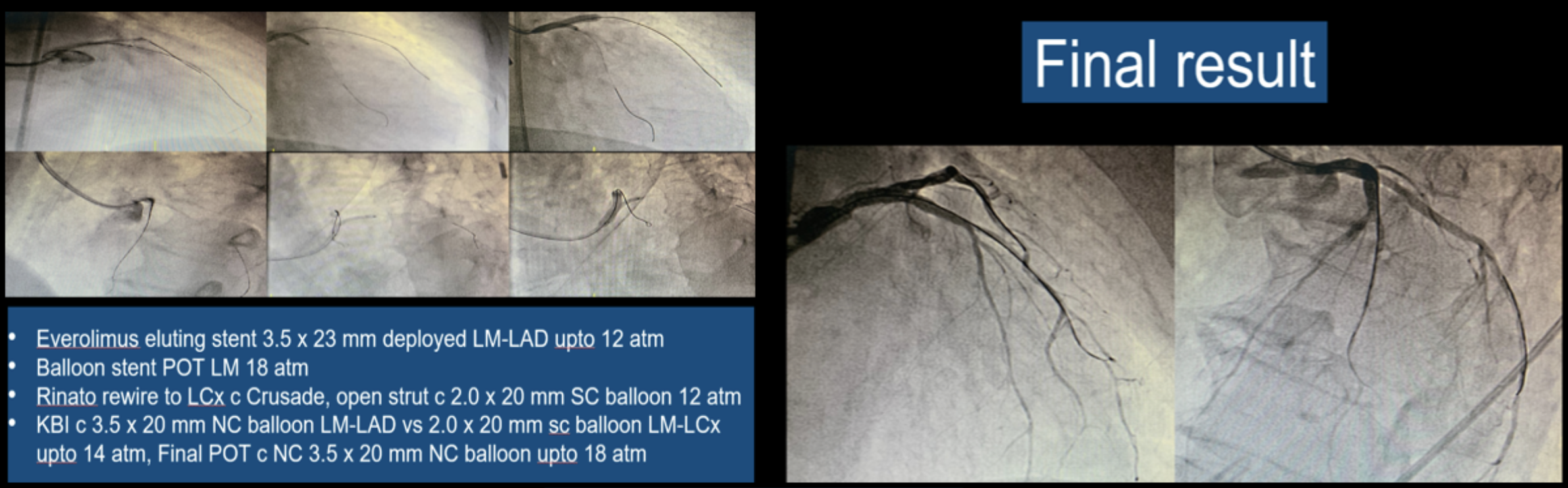
What is the best strategy revascularization for critical ostial LM-LAD? (1. CABG 2. Inserted IABP c PCI LM-LAD, Which technique? 3. PCI LM-LAD, Which technique? 4. Other options? ). PCI LM-LAD via Right femoral approach 7 Fr sheath with Short tip JL 3.5/7 Fr guiding catheter to LCA. Rinato for floating wire technique, Fielder XT try to pass through LM. Fielder XT pass through LM subintima. The patient developed chest discomfort and blood pressure drop 84/47 mmhg. The patient was given inotrope and IABP support. What will you do next? (1. Consult CVT for emergency CABG 2. Reattempt PCI LM-LAD 3. Medication treatment 4.Other options?). Try reattempt PCILM-LAD. Fielder XT can cross LM through LCx, SC balloon 2.0 x 20 mm inflated LM-LCx upto12 atm, Rinato pass to LM-LCx, move Fielder XT to LAD, Predilate LM-LAD c 2.0 x 20 mm SC balloon upto 12 atm, 3.5 x 20 mm NC balloon upto 24 atm, Everolimus eluting stent 3.5 x 23 mm deployed LM-LAD upto 12 atm, Balloon stent POT LM 18 atm, Rinato rewire to LCx c Crusade, open strut c2.0 x 20 mm SC balloon 12 atm, KBI c 3.5 x 20 mm NC balloon LM-LAD vs 2.0 x20 mm sc balloon LM-LCx upto 14 atm, Final POT c NC 3.5 x 20 mm NC balloon upto18 atm. The final angiogram was acceptable result.

Case Summary
1.Clinical, anatomic, and procedural factors should be taken into account when selecting the mode of revascularization for LM disease2.IABP implantation can provide additional hemodynamic support in high risk PCI, particularly Low SBP, RCA stenosis, severely reduced LVEF