
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-142
Successful Percutaneous Coronary Intervention of Catheter Induced Type F Coronary Artery Dissection With Subintimal Tracking and Re-Entry Technique.
By Chong Wei Loong, Khoo Song Weng Ryan, Chew Fui Lo, Neerusha Kaisbain, Houng Bang Liew
Presenter
Chong Wei Loong
Authors
Chong Wei Loong1, Khoo Song Weng Ryan2, Chew Fui Lo2, Neerusha Kaisbain2, Houng Bang Liew2
Affiliation
KPJ Sabah Specialist Hospital, Malaysia1, Queen Elizabeth II Hospital, Malaysia2,
View Study Report
TCTAP C-142
Coronary - Complication Management
Successful Percutaneous Coronary Intervention of Catheter Induced Type F Coronary Artery Dissection With Subintimal Tracking and Re-Entry Technique.
Chong Wei Loong1, Khoo Song Weng Ryan2, Chew Fui Lo2, Neerusha Kaisbain2, Houng Bang Liew2
KPJ Sabah Specialist Hospital, Malaysia1, Queen Elizabeth II Hospital, Malaysia2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
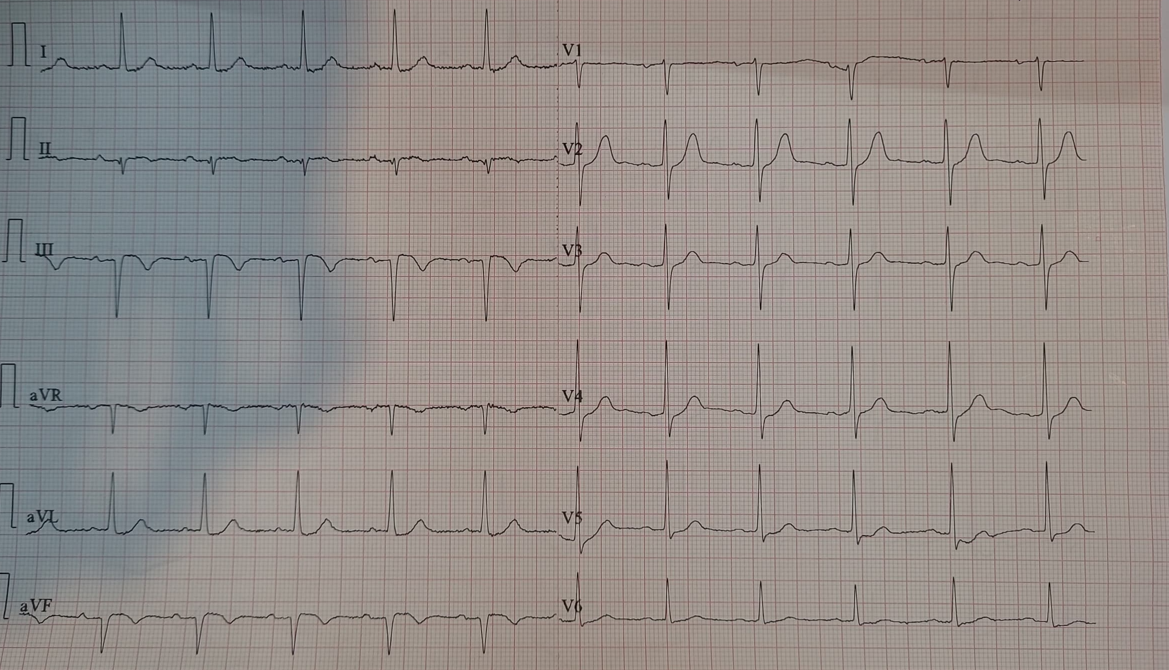
A 54 year old man with underlying hypertension and history of inferior myocardial infarction 2 months ago presented with recurrent chest pain at rest. His blood pressure on arrival was 200/110mmHg. Cardiovascular and respiratory examination were unremarkable. Electrocardiography showed Q waves of the inferior leads. Echocardiography showed preserved left ventricular ejection fraction with inferior wall hypokinesia. His cardiac troponin was normal.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
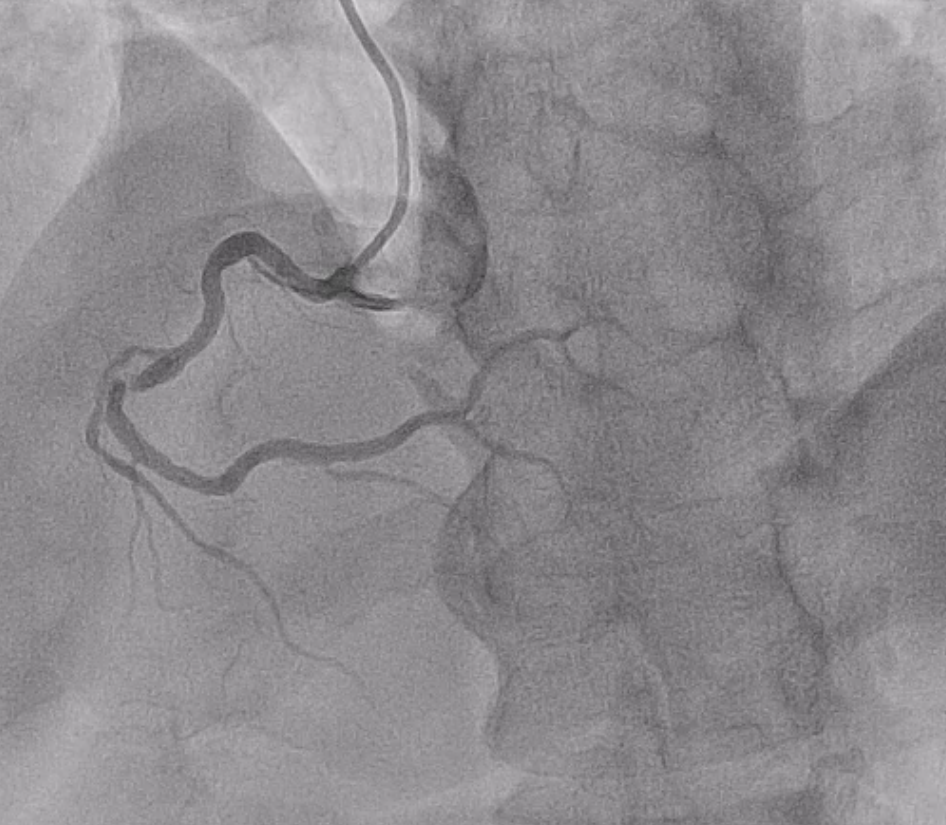
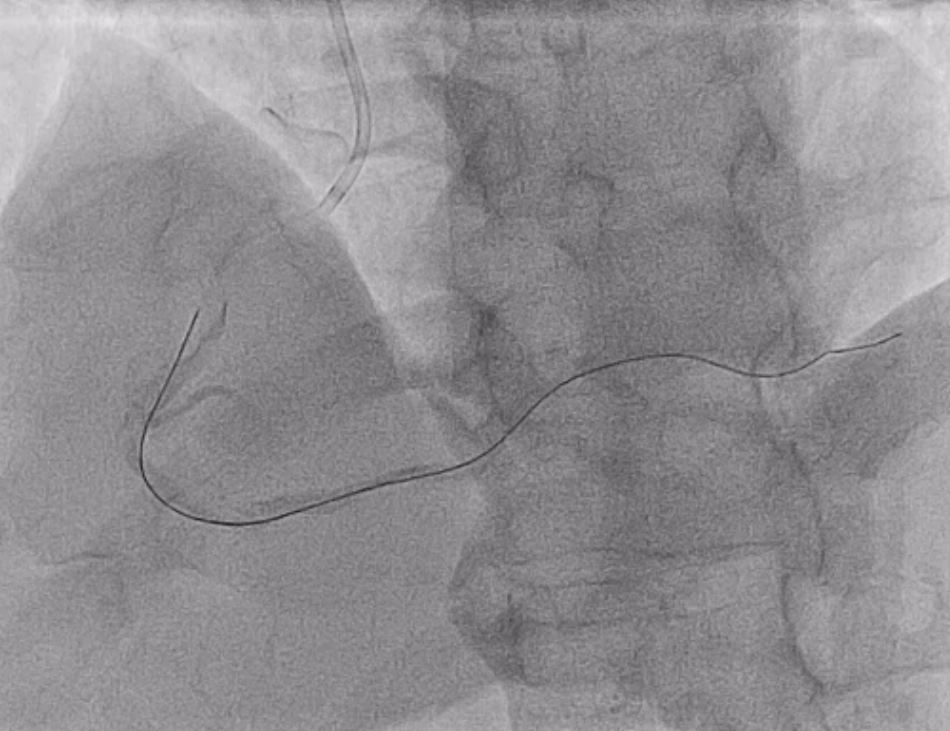
Diagnostic coronary angiography with Optitorque catheter showed mid left anterior descending artery stenosis and severe stenosis of the mid right coronary artery. Decision to proceed with percutaneous coronary intervention of the right coronary artery. 6Fr Judkins Right 4 guiding catheter engaged right coronary artery and coronary angiography revealed Type F dissection of the ostial right coronary artery with TIMI 0 flow.

Interventional Management
Procedural Step
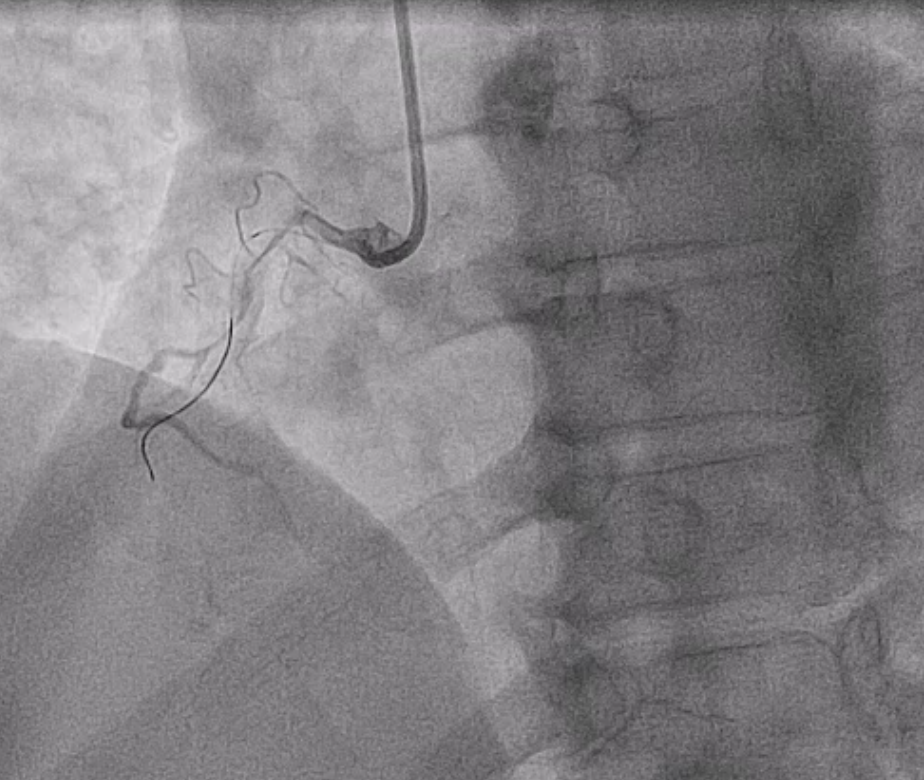
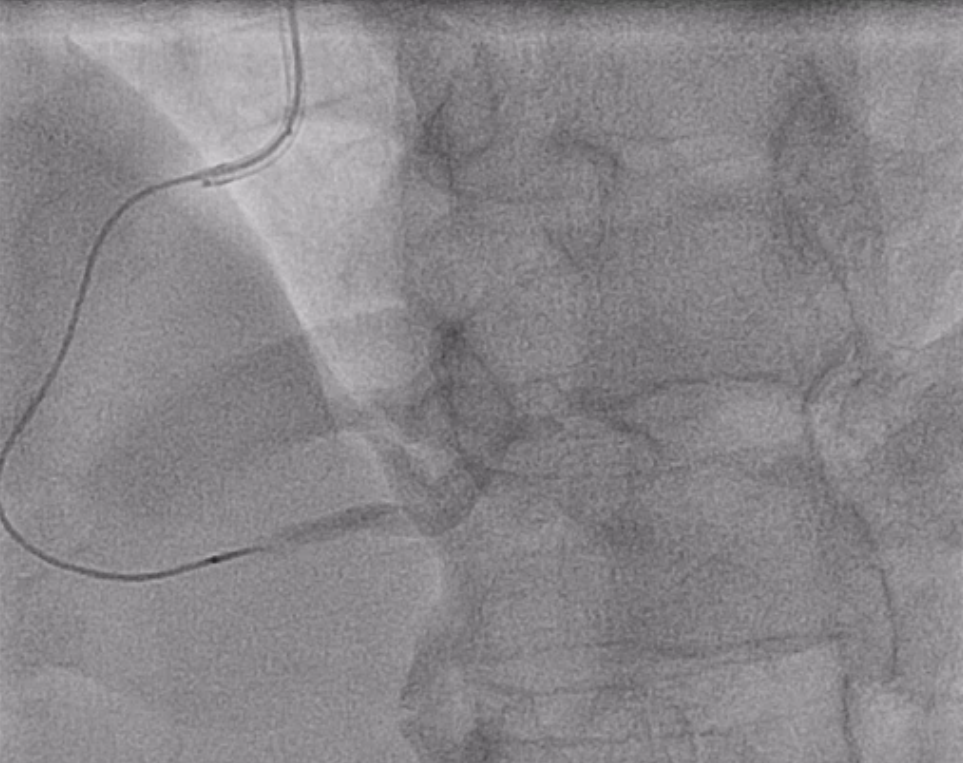
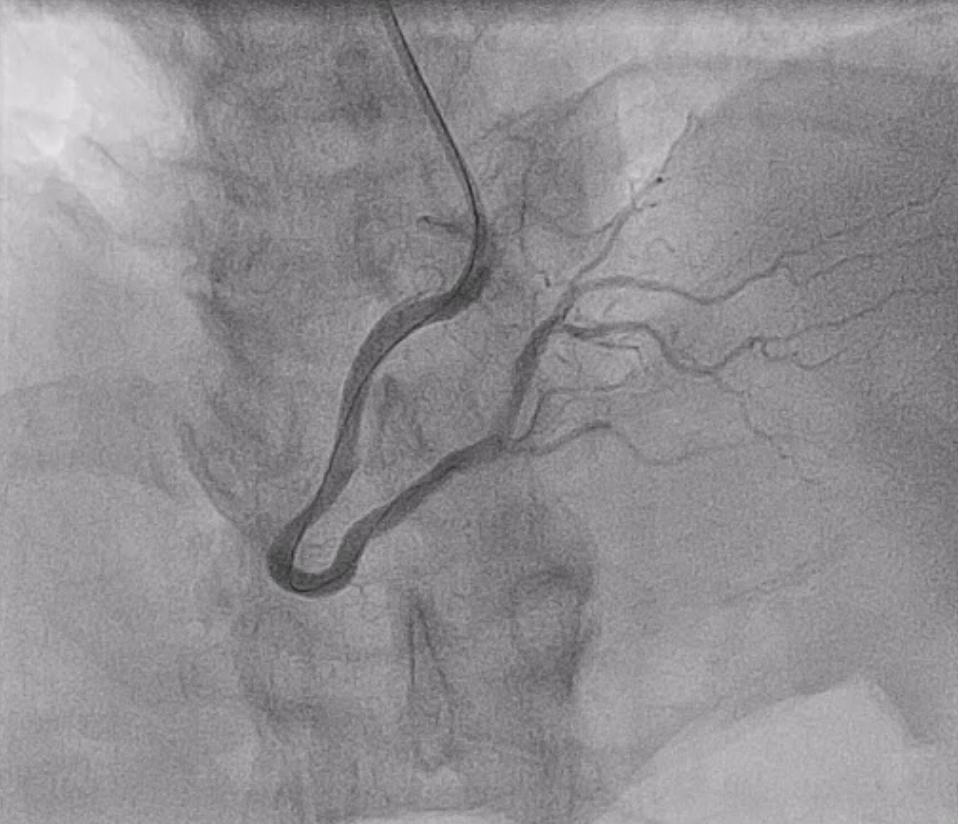
During the procedure, patient complained of chest pain with ST elevation. We were unable to wire the Balance Middle Weight and Pilot 50 guidewires into the true lumen. Gaia First guidewire was advanced through the subintimal space to the distal crux and entered the posterior lateral artery. A Corsair Pro microcatheter was placed at the distal right coronary artery. After removing the guidewire, 2ml of contrast was injected through the microcatheter and the distal true lumen of posterior lateral artery was visualized. By using contrast guided subintimal tracking and re-entry technique, a low tip load, polymer jacketed Fielder XTR guidewire was advanced into the true lumen of distal posterior lateral artery. Pre-dilatation performed with semi compliant Sapphire balloon 2.0x15mm at 6atm. Four overlapping drug eluting stents (Resolute Onyx 3.0x36mm,Resolute Onyx 3.0x26mm, Resolute Onyx 3.0x22mm, Resolute Onyx 30x26mm) were implanted from the right coronary artery ostium to the distal crux. Post-dilatation performed with a non compliant Sapphire balloon 3.5x15mm at 18atm. TIMI 3 flow established.
Case Summary
Catheter induced coronary artery dissection is a rare but potentially life threatening complication of cardiac catheterization. Type F coronary dissection requires timely recognition and bailout strategy. If the guidewire is in the false lumen, subintimal tracking and re-entry technique into the distal true lumen followed by subintimal stenting is a feasible bailout option.