
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-034
Halfway Rotational Atherectomy With Cutting Balloon to Facilitation of PCI at Very Tortuous LAD
By Osit Bambat
Presenter
Osit Bambat
Authors
Osit Bambat1
Affiliation
Chiangrai Prachanukroh Hospital, Thailand1,
View Study Report
TCTAP C-034
Coronary - Complex PCI - Calcified Lesion
Halfway Rotational Atherectomy With Cutting Balloon to Facilitation of PCI at Very Tortuous LAD
Osit Bambat1
Chiangrai Prachanukroh Hospital, Thailand1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
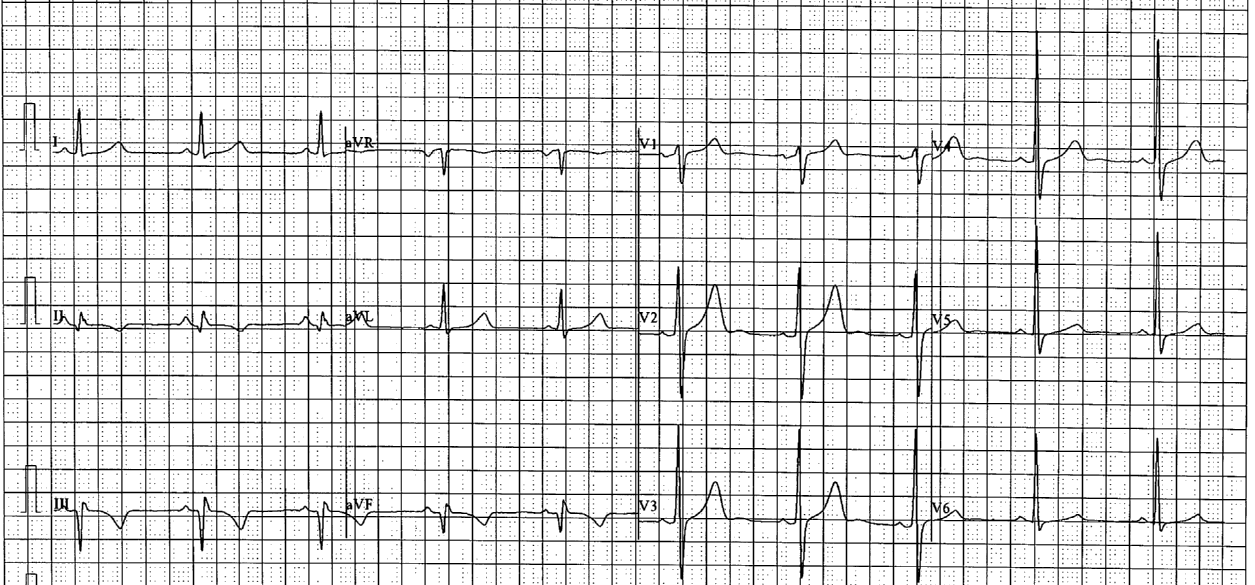
A 55 years old man underlying type 2 diabetes, hypertension and hypertriglyceridemia had chest pain for 2 hours. He went to the rural hospital and diagnosed acute STEMI inferior wall. Streptokinase was given and ECG showed complete resolution. He was referred for pharmacoinvasive strategy. CAG showed triple vessel disease. He denied CABG and was scheduled for staged PCI at LAD.

Relevant Test Results Prior to Catheterization
Hct 36.6%, Creatinine 0.85 mg/dl, eGFR 96, FBS 165 mg%, HbA1C 7.6%, cholesterol 285 mg/dl, triglyceride 1800 mg/dl, HDL 41 mg/dl, direct LDL 58 mg/dlChest X-ray : no cardiomegaly, no pulmonary congestionECG : normal sinus rhythm, Q at inferior leads, LVH by voltageEcho : LVEF 54%, hypokinesia at inferior wall, mild MR
Relevant Catheterization Findings
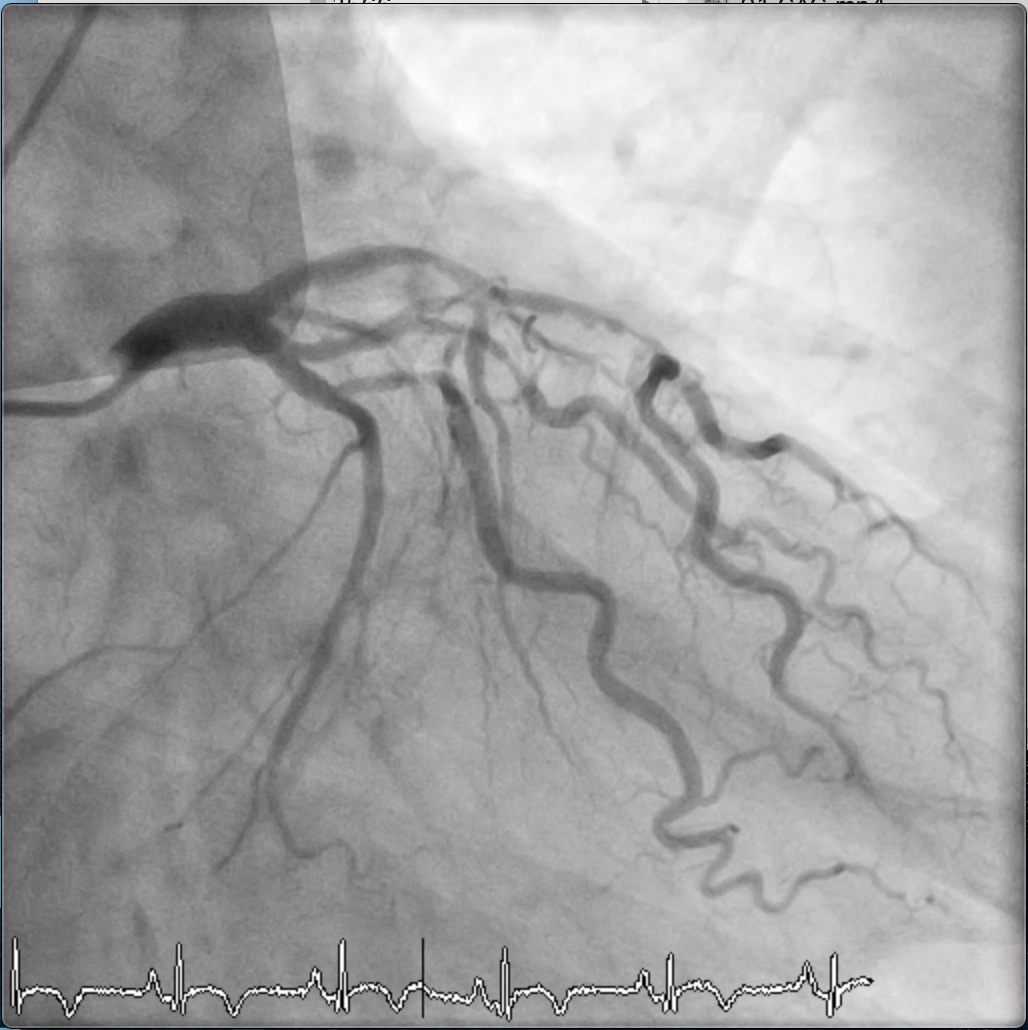
CAG revealed a very tortuous LAD with tight calcification lesions at proximal and mid LAD. LCX had borderline stenosis at both proximal OM1 and OM2. RCA had severe stenosis at mid and distal parts.


Interventional Management
Procedural Step
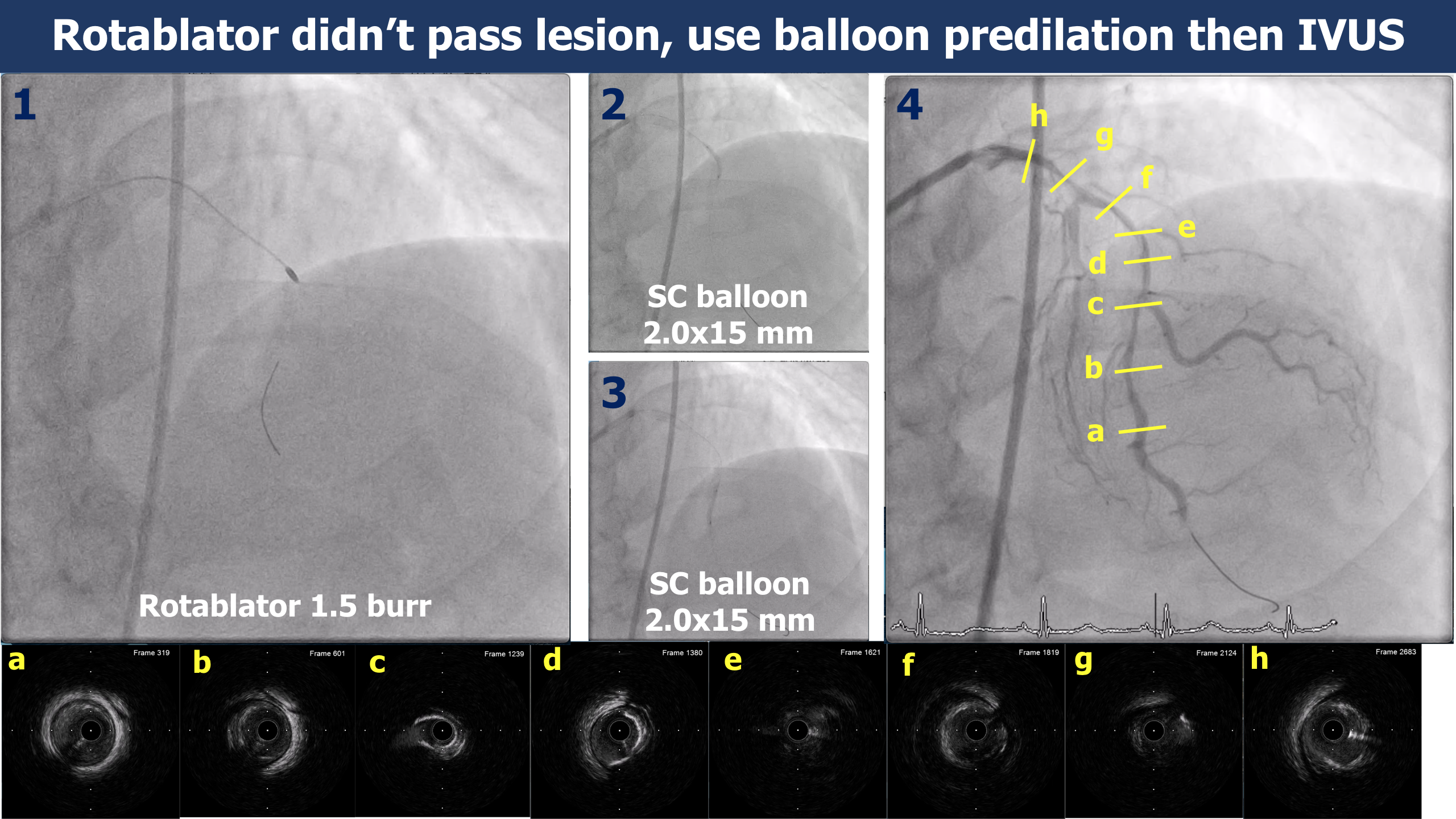
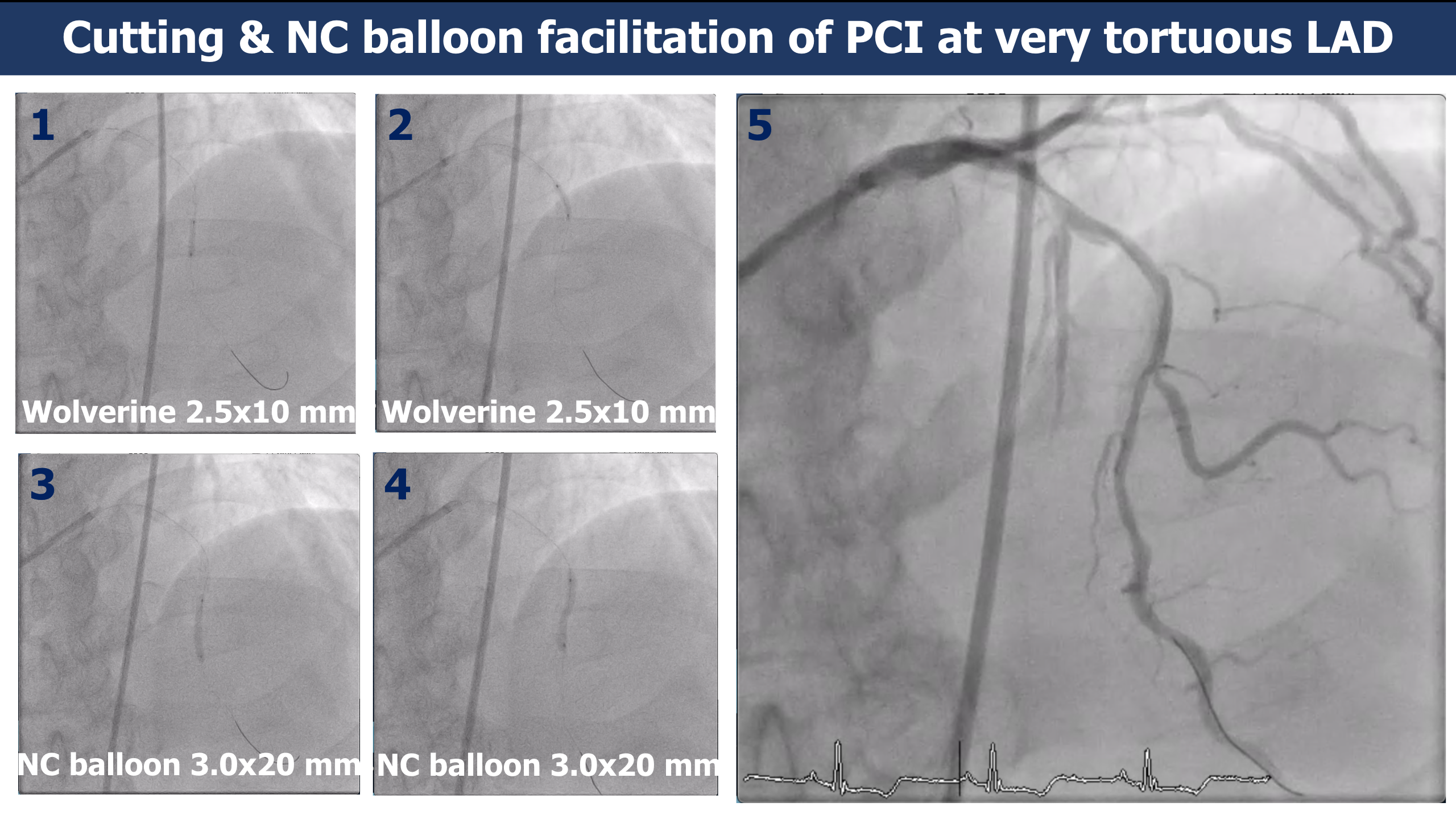
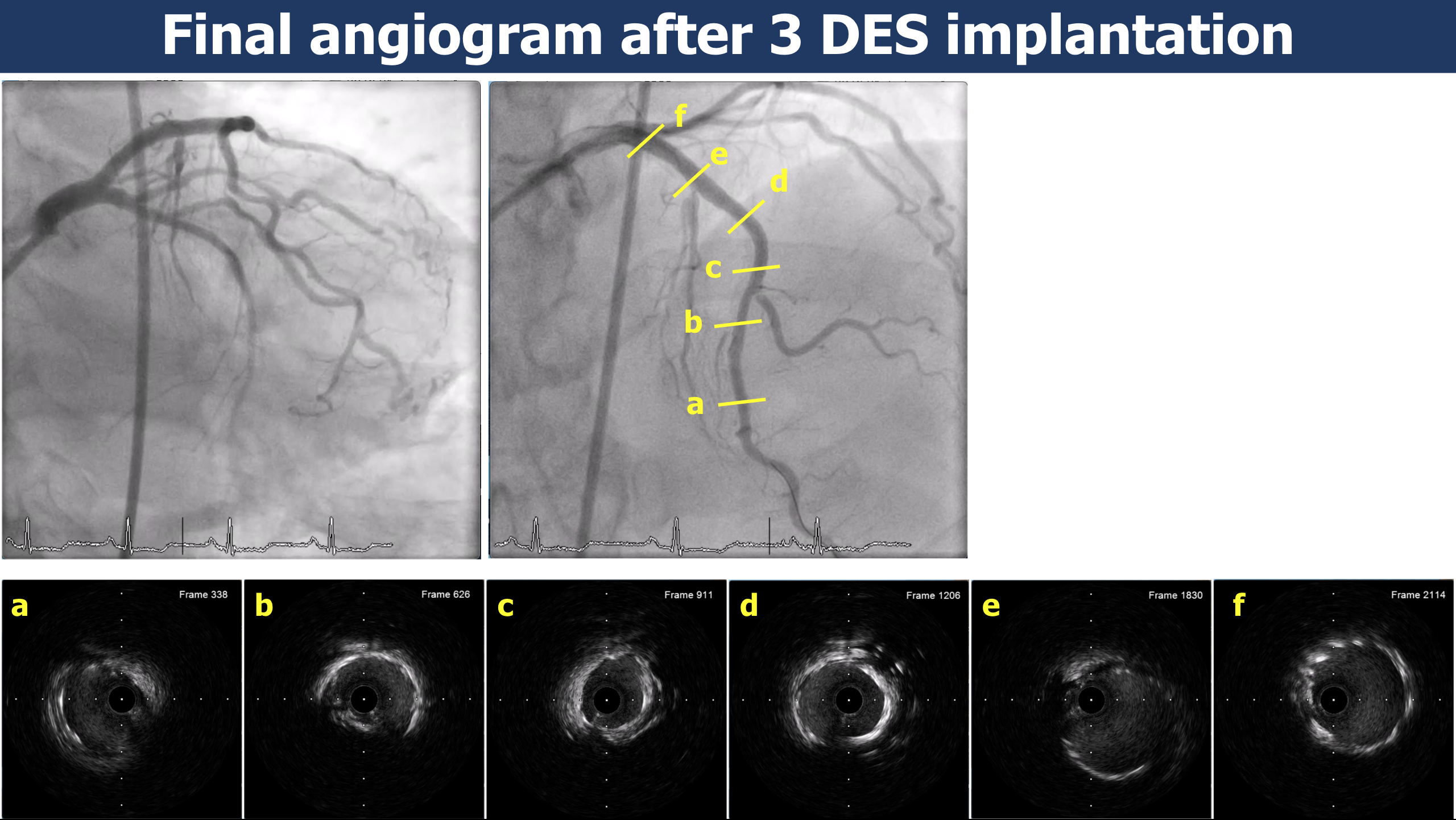
Rotational atherectomy 1.5 burr was done on rota floppy wire. The first lesion at proximal LAD was successfully ablated in 1 time but the rotablator can not pass the very tortuous mid LAD lesion after 4 times. Guidewire was exchanged to Sion Blue wire and semi-compliant balloon 2.0x 15 mm was used for predilatation. IVUS showed 180 degree calcification with fibrocalcific plaque at proximal LAD and nearly 360 degree of calcification and very severe stenosis at mid LAD. To avoid the rotational atherectomy cut through of the coronary vessel, Wolverine cutting balloon 2.5x 10 mm was used instead for calcium modulation at mid LAD. Then non-compliant balloon 3.0x 20 mm was used for predilatation again. The angiogram after POBA showed good lesion preparation and coronary dissection along proximal to distal LAD. The 3.0x 36 mm and 3.5x24 mm DES were deployed at distal and mid LAD respectively. The last 4.0x 24 mm DES was deployed at proximal LAD. IVUS showed both stents were underexpansion then used non-compliant balloons 3.5x 15 mm and 4.0x 20 mm were inflated at high pressure for post dilatation. The final angiogram and IVUS showed acceptable stent expansion without complications.
Case Summary
Rotational atherectomy in a very tortuous coronary vessel must be used with high caution. If the rotablator can’t pass the tortuous lesion, other options such as a cutting balloon or NC balloon could be used safely to avoid coronary perforation.