
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-203
EKOS in IVC Thrombosis
By Li-Hao Yap, Mu Shang Huang
Presenter
Li-Hao Yap
Authors
Li-Hao Yap1, Mu Shang Huang2
Affiliation
National Cheng Kung University Hospital, Ta, Taiwan1, National Cheng Kung University Hospital, Taiwan2,
View Study Report
TCTAP C-203
Endovascular - Thrombus Removal Devices and Techniques
EKOS in IVC Thrombosis
Li-Hao Yap1, Mu Shang Huang2
National Cheng Kung University Hospital, Ta, Taiwan1, National Cheng Kung University Hospital, Taiwan2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 48-year-old woman with underlying diseases of primary antiphospholipid syndrome, presented with abdominal pain and left leg swelling for weeks. Physical exam showed diffuse abdominal tenderness without muscle guarding or rebounding pain, bilateral lower extremities pitting edema (3+), especially left leg.
Relevant Test Results Prior to Catheterization
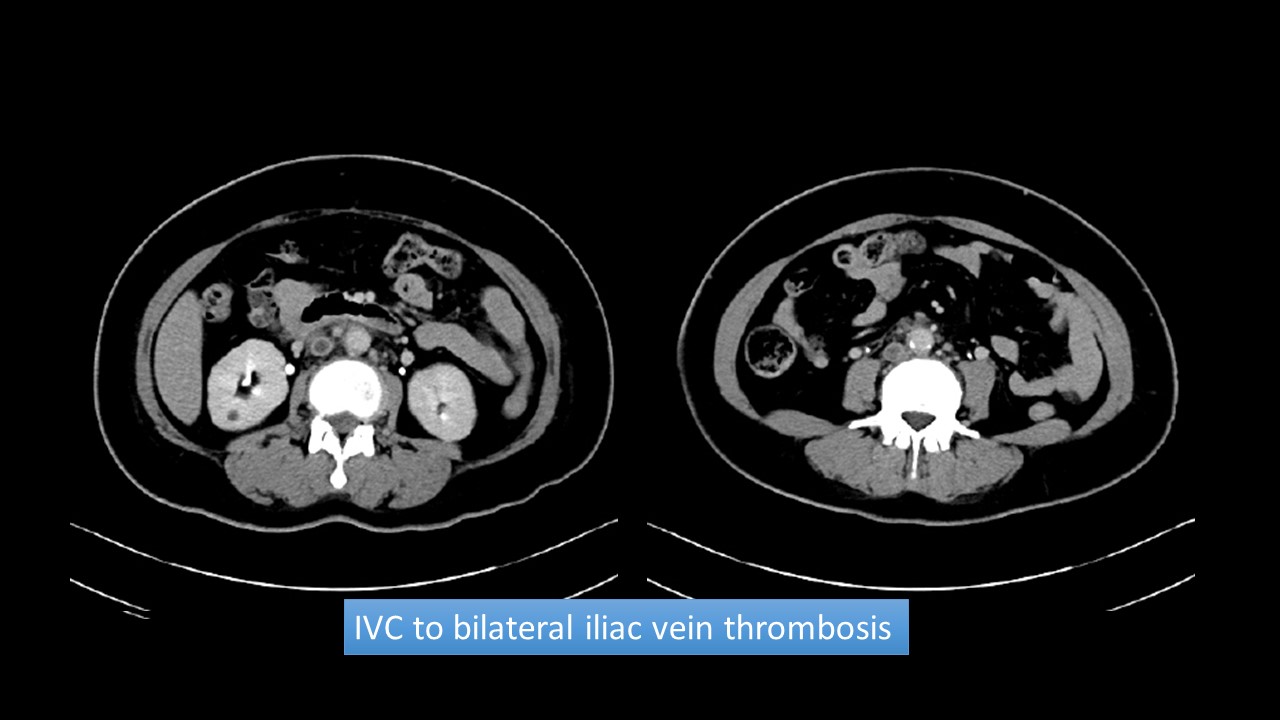
Abdomen CT (with/without contrast) revealed IVC to bilateral iliac vein thrombosis. No abdominal/pelvic tumor was noted.

Relevant Catheterization Findings
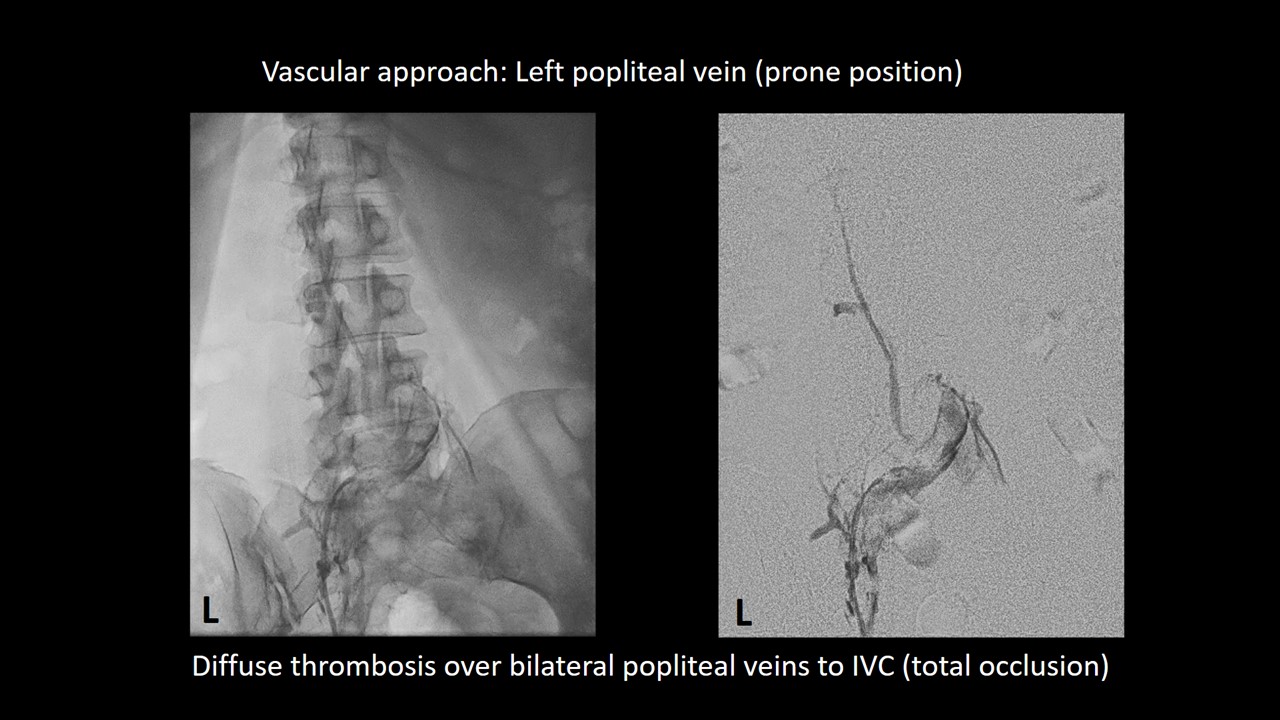
Via left popliteal venous access, venography showed abundant thrombus formation, from left popliteal vein up to IVC.
Interventional Management
Procedural Step
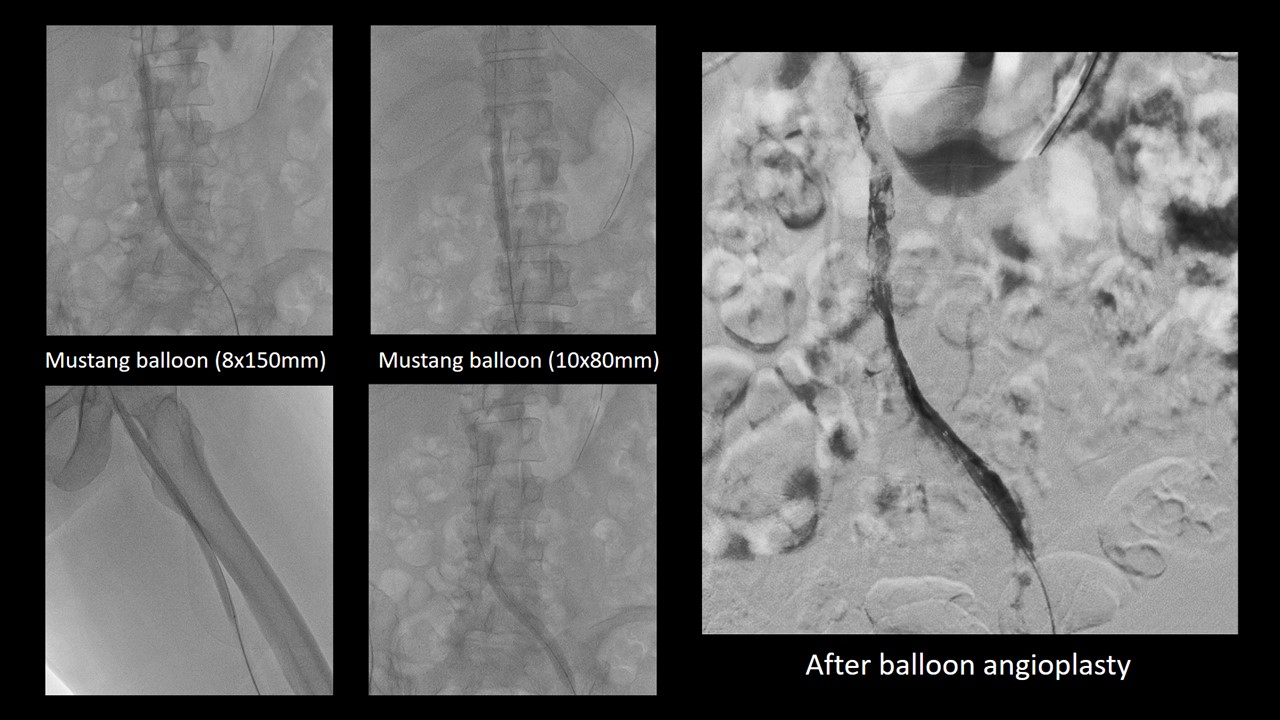
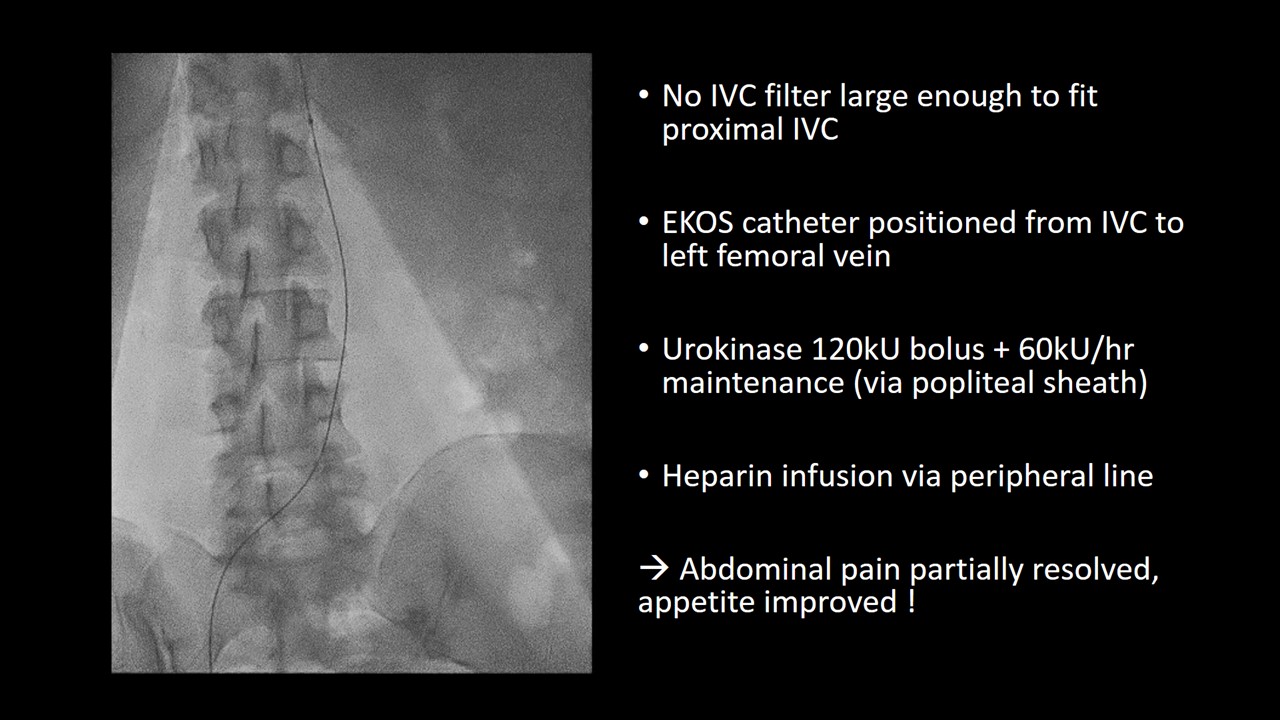
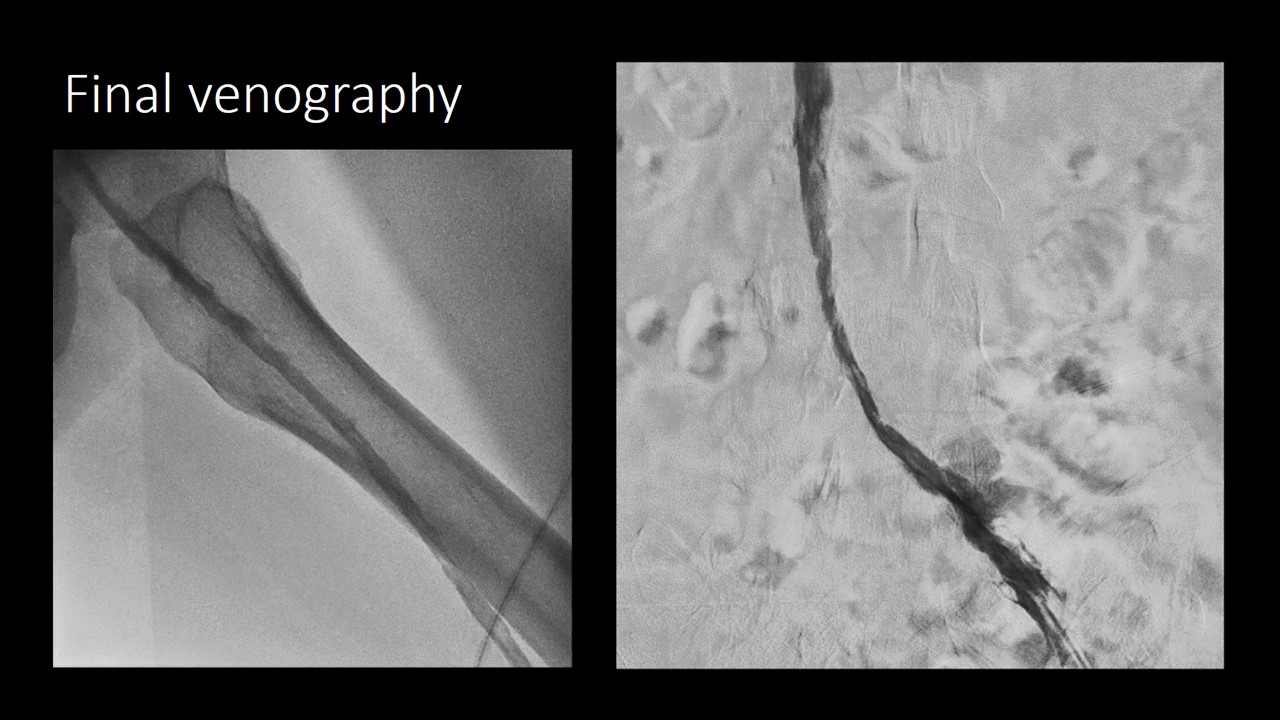
After venography, EKOS catheter was inserted via left popliteal vein, positioned from left femoral vein to IVC. No IVC filter large enough to fit proximal IVC was available, so IVC filter was not implanted. Urokinase (bolus 120000U, maintenance 60000U/hr) was given via infusion catheter. Heparinization via peripheral IV line was also administered. In the following days, patient reported markedly improvement of abdominal pain and appetite. Follow-up venography showed partial resolution of thrombus over IVC to left femoral vein.Balloon angioplasty (8mm, 10mm) was done, then infusion catheter (Fountain,4Fr, 40cm) was placed over IVC to left femoral vein for 4 more days. Final venography showed patent IVC and femoral vein flow. Symptoms resolved completely,no pulmonary embolism or major bleeding was reported.
Case Summary
• EKOS provides a effective,promising treatment for IVC thrombosis