
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-159
Chip-PCI in a 63-Year-Old Female Patient With HFrEF. Are These Lesions Chronic and Stable?
By Hsuan I Pan
Presenter
Hsuan I Pan
Authors
Hsuan I Pan1
Affiliation
Kaohsiung Medical University Chung-Ho Memorial Hospital, Taiwan1,
View Study Report
TCTAP C-159
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
Chip-PCI in a 63-Year-Old Female Patient With HFrEF. Are These Lesions Chronic and Stable?
Hsuan I Pan1
Kaohsiung Medical University Chung-Ho Memorial Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
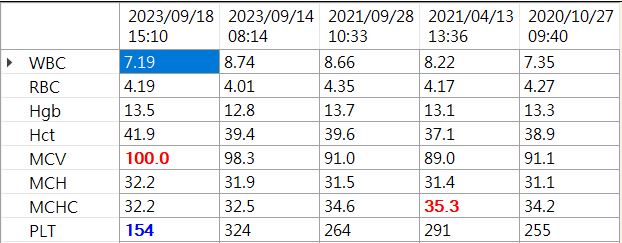
This 63-year-old woman, previously treated for breast cancer, was admitted to our ward on September 18, 2023, due to exertional dyspnea. Accompanying symptoms included bilateral lower limb edema and tachycardia. Upon physical examination, crackles were noted over the bilateral basal lung areas. Laboratory results indicated no anemia and normal renal function, but there was an elevation in B-type natriuretic peptide levels and a slight increase in troponin I.


Relevant Test Results Prior to Catheterization
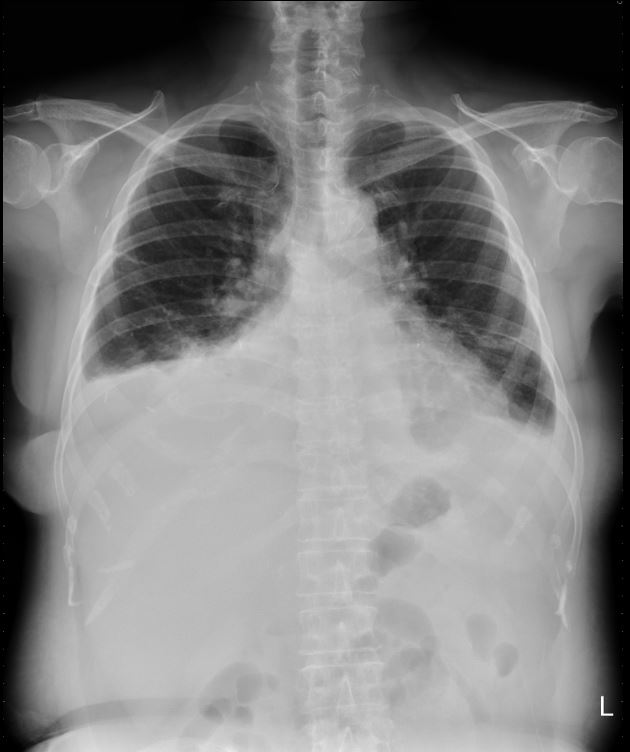
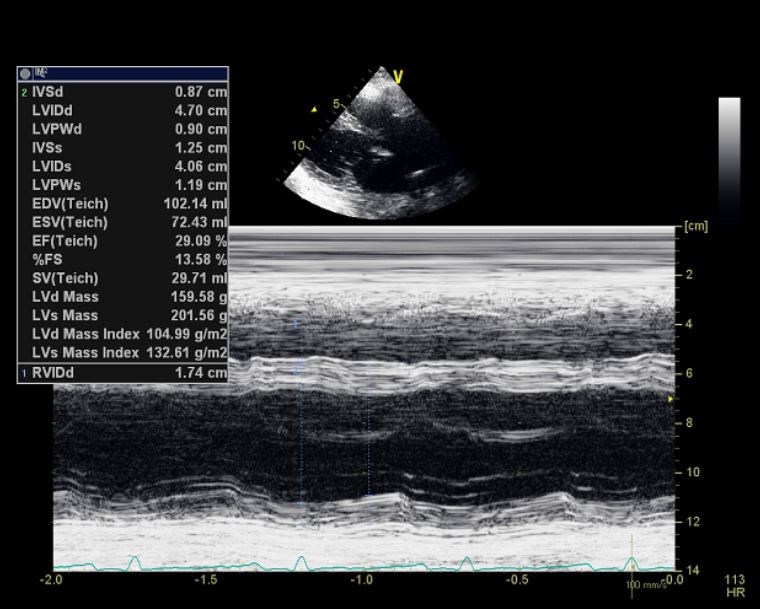
Electrocardiography showed sinus tachycardia without obvious ST-T change.Chest X ray showed right side pleural effusionCardiac echo showed impaired global left ventricular systolic function, Biplalne LVEF 24.8%, Moderate mitral valve regurgitation and tricuspid valve regurgitation.

Relevant Catheterization Findings
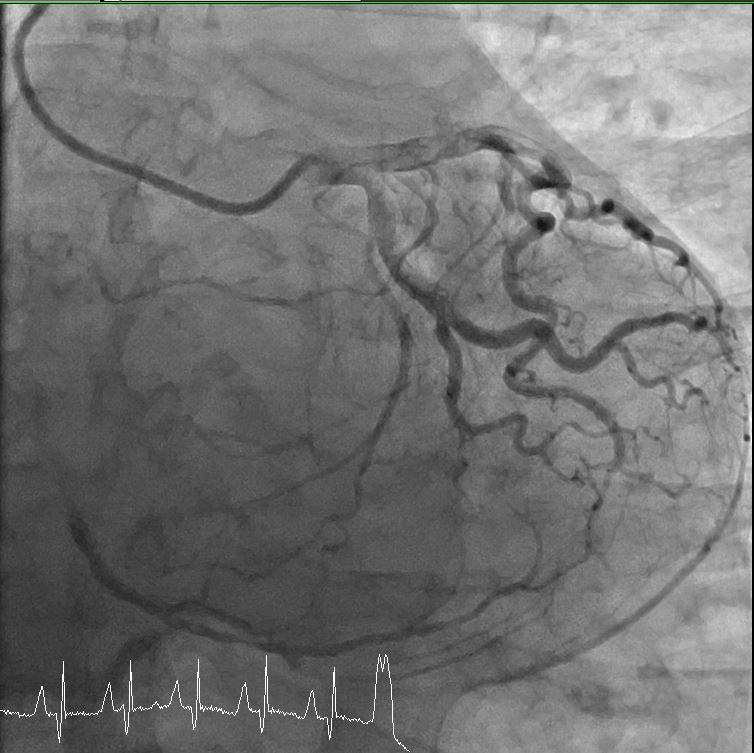
left main coronary artery: no stenosisright coronary artery : Seg1 100% stenosis, large thrombus burden, with collateral from left anterior descendingleft anterior descending : Mid 30% stenosisleft circumflex artery: no stenosis


Interventional Management
Procedural Step
-RCA Guiding catheter: (Medtronic) PTCA Guiding Catheter[7F SAL.75]. Guide Wire2: (Terumo) RUNTHROUGH NS PTCA GUIDE WIRE[Hypercoat 180cm]. Aspiration catheter: (Goodman) REBIRTH PRO2 Theombus ASpiration Catheter[7Fr].** We use hypercoat pass 100% stenosis at RCA--- Predilation and thrombectomy Balloon: (TERUMO) Ryurei PTCA Dilatation Catheter[1.5mmx15mm]. Pressure: 6 atmospheres. Balloon2: (TERUMO) Ryurei PTCA Dilatation Catheter[2.0mmx40mm]. Pressure: 6 atmospheres.** We also check IVUS at RCA after predilation and thrombectomy and Aggrastat use** Then, we use "self-paid thrombus filter(spider) use" at RCA for distal run off protection --- Stenting Stent: (Boston) SYNERGY EVEROLIMUS-ELUTING CORONARY STENT SYSTEM[3.0mmx48mm]. Pressure: 16 atmospheres.--- Post dilation Balloon3: (Terumo) ACCUFORCE PTCA BALLOON DILATATION CATHETER[3.0mmx15mm]. Pressure: 12 atmospheres. Balloon4: (Terumo) ACCUFORCE PTCA BALLOON DILATATION CATHETER[3.5mmx20mm]. Pressure: 12-20 atmospheres. Balloon5: (Terumo) ACCUFORCE PTCA BALLOON DILATATION CATHETER[4.0mmx20mm]. Pressure: 4-16 atmospheres.



Case Summary
This is a case of heart failure with reduced ejection fraction, notable for the absence of chest pain and no history of diabetes mellitus. The condition is suspected to be linked to a recent myocardial infarction.Coronary angiography revealed signs suggestive of a recent myocardial infarction and identified 1-vessel coronary artery disease. The patient underwent successful revascularization through the placement of a drug-eluting stent, along with thrombectomy and the use of a filter at the right coronary artery, accompanied by the administration of Tirofiban.Following the revascularization procedure on the right coronary artery, there was a notable improvement in dyspnea on exertion.