
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-147
Primary Angioplasty With Hybrid Approach Using Drug-Eluting Stent and Drug-Coated Balloon.
By Kalyanaraman Kannan
Presenter
Kalyanaraman Kannan
Authors
Kalyanaraman Kannan1
Affiliation
Kalyaan Speciality Hospital, India1,
View Study Report
TCTAP C-147
Coronary - DES/BRS/DCB
Primary Angioplasty With Hybrid Approach Using Drug-Eluting Stent and Drug-Coated Balloon.
Kalyanaraman Kannan1
Kalyaan Speciality Hospital, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 62-year-old male with diabetes mellitus came to our hospital with chest pain of 2 hours associated with sweating. On arrival to the emergency room, his vital were stable. He was given a loading dose of ecosprin 325 mg, ticagrelor 180 mg, and atorvastatin 40 mg and immediately shifted to the catheterisation lab in 10 minutes.

Relevant Test Results Prior to Catheterization
ECG acute inferior wall myocardial infarction

Relevant Catheterization Findings
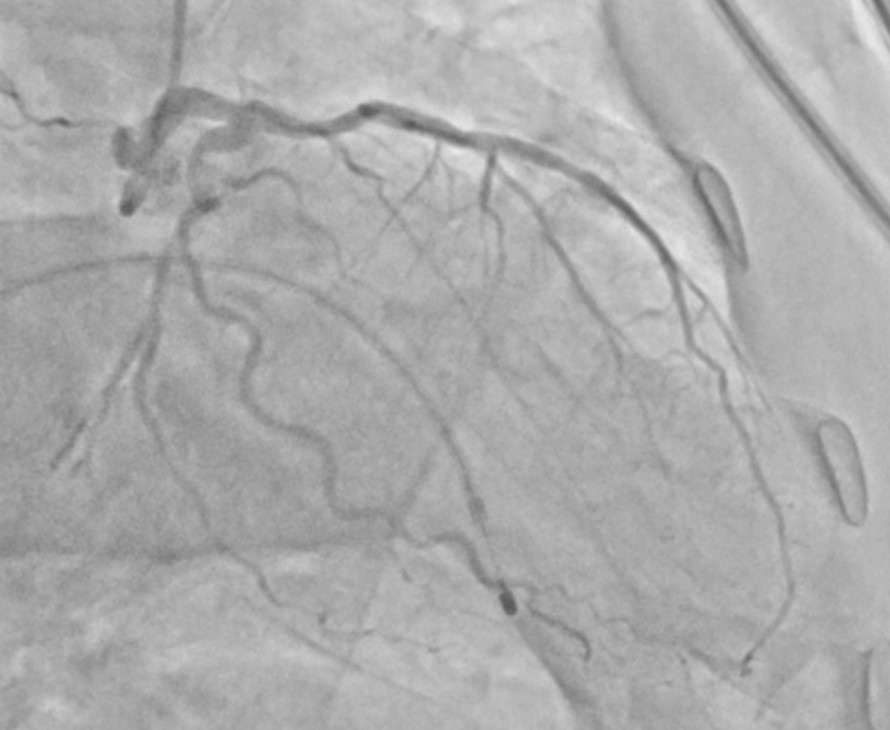
A coronary angiogram was done through the right femoral approach using a 6F sheath, 6F Judkins right, and 6F Judkins left diagnostic catheter. Immediately after femoral puncture, he developed repeated episodes of ventricular fibrillation. Cardiopulmonary resuscitation was done with DC shock around 12 times and temporary pacemaker support. After stabilising the patient, an angiogram was done.Coronary angiogram findings

Interventional Management
Procedural Step
RCA was engaged with 6 Fr Judkins 3.5 guiding catheter; the proximal RCA lesion was pre-dilated with (1.5 x 10 mm) SC balloon at 12 atm for 20 seconds and pre-dilated with (2.0 x 8 mm) NC balloon at 14 atm for 20 seconds, the (2.0x 15 mm) resolute onyx stent was deployed at 16 atm for 30 seconds. Post-dilation was done with a 2.5 x 12 mm NC balloon at 16 atm for 30 seconds. The distal RCA lesion was pre-dilated with (2.0x 8 mm) NC balloon at 12 atm for 20 seconds after crossing with the buddy wire technique. Subsequently, the (2.5 x 15) sirolimus-coated drug-eluting balloon was inflated at 10 atm for 60 seconds. The final angiogram showed a well-deployed stent with a good approximation of the proximal RCA stent and complete expansion of distal RCA with TIMI III flow in the right coronary system. The patient was shifted to the ICU with stable hemodynamics.



Case Summary
This case highlights the importance of a drug-coated balloon when two lesions are in the same vessel. Even during primary percutaneous intervention in acute coronary syndrome, critical lesions can be stented, and lesions in distal vessels and small branches can be dilated with a drug-coated balloon. There is a good outcome due to the possibility of future positive remodelling. We can avoid unnecessary use of multiple stents in the same patient.