
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-137
A Challenging Bail Out in an Unexpected Case of Stent Distortion
By Purushottam Kumar
Presenter
Purushottam Kumar
Authors
Purushottam Kumar1
Affiliation
Prashant Memorial Charitable Hospital, India1,
View Study Report
TCTAP C-137
Coronary - Complication Management
A Challenging Bail Out in an Unexpected Case of Stent Distortion
Purushottam Kumar1
Prashant Memorial Charitable Hospital, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
61 years old female non diabetic, hypertensive strong family history of CAD presented in OPD with Class III angina.Patient had stable hemodynamics unremarkable cardiorespiratory examination, non contributory labs.Ecg reveled T wave inversion in inferolateral leads.Echo showed concentric LVH,EF 65%,No RWMA at rest.

Relevant Test Results Prior to Catheterization
Ecg Inferolateral ischemiaEcho LVEF 65% Concentric LVH CVS S1S2+ RS A/EB/L+ VBS+Hb 13.5g/dl creatinine 0.9 Viral markers negative
Relevant Catheterization Findings
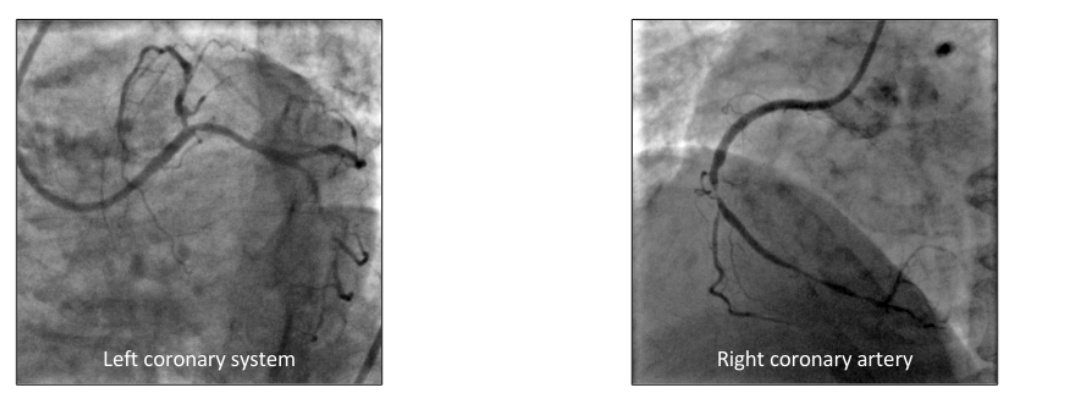
Coronary Angiography revealed Triple Vessel Coronary Artery DiseaseLeft Main-NormalLeft Anterior Descending-Ostial 70%,mid-distal 90%Left circumflex-Non dominant,Mid distal 90%Right Coronary artery-Dominant,mid 90%,Distal 90%
Patient refused CABG and opted for a multivessel PCIIntervention to LAD and RCA where planned
Patient refused CABG and opted for a multivessel PCIIntervention to LAD and RCA where planned
Interventional Management
Procedural Step
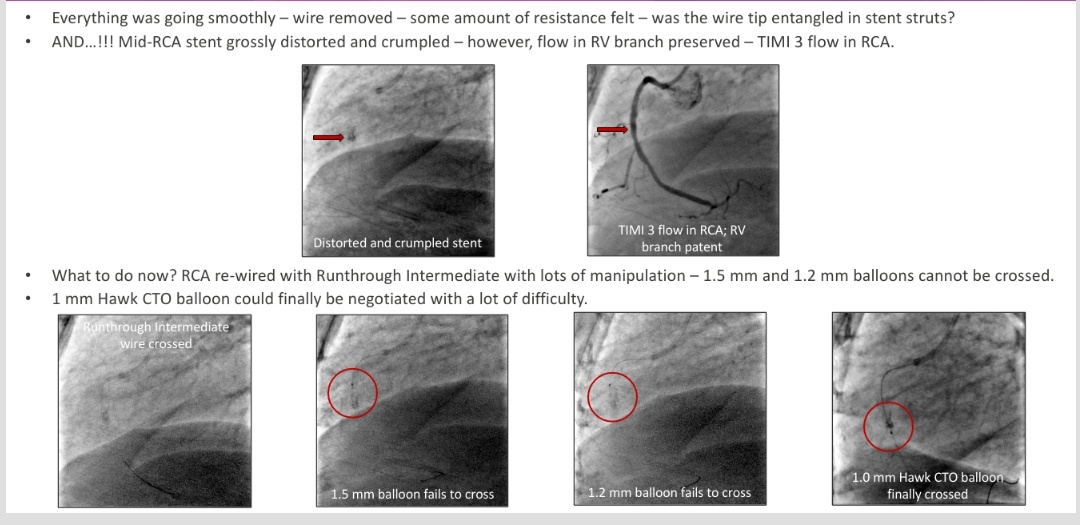
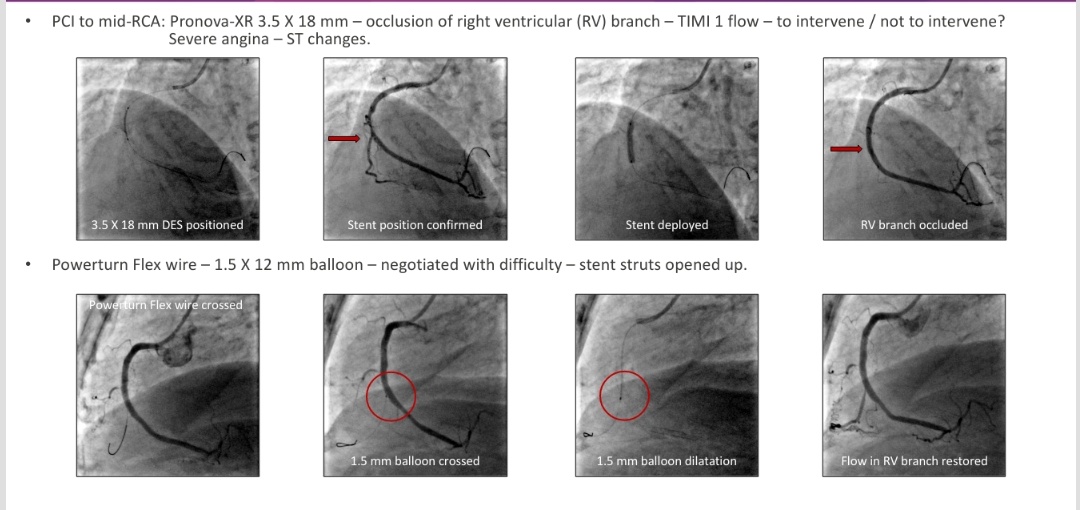
Uncomplicated PCI to LAD and distal RCA was done. PCI to LAD was done through Femoral access with 7 Fr XB 3.5 guide catheter-Sion blue wire and PCI to distal RCA was done Femoral access with 7 Fr 3.5 guide catheter-Sion blue wire.PCI to mid RCA was done And Pronova XB 3.5 X 18 mm was used and TIMI III flow in RCA was achieved but in due course RV branch got occluded with TIMI I flow and patient had severe Angina.Wire was crossed to RV branch and 1.5MM x 12 mm balloon was crossed and flow restored. Everything was going smoothly and as wire was removed there was some resistance felt in stent struts and wire got entangled in stent struts, Mid RCA stent got grossly distorted and crumpled. RCA was rewired and lots of manipulation was done and with lots of difficulty 1mm Hawk CTO balloon crossed and serial pre dilatation with 1.0 mm,2.5 mm,3.0 mm non compliant balloon to appose distorted stent struts and Pronova 3.5 MM X 28 MM stent deployed.Acceptable final result was attained with TIMI III flow in the RCA.

Case Summary
The decision to intervene into side branches requires careful deliberation. Coronary wires get entangled into stent struts and should never be withdrawn against resistance.If required alternate techniques such as pushing balloon or micro catheter over it should be tried.
Methods of extraction of retained wire fragment:-1)Double or Triple wire technique2)Deep wedging of guiding catheter and traction of the system3)Removal using Balloon inflation technique4)Retrieval by snare loop5)Retrieval using micro catheter6)Extraction with Bioptome
Finally, we achieved TIMI III flow and patient is completely asymptomatic and we plan a repeat coronary angiography for the patient after 6 months.
Methods of extraction of retained wire fragment:-1)Double or Triple wire technique2)Deep wedging of guiding catheter and traction of the system3)Removal using Balloon inflation technique4)Retrieval by snare loop5)Retrieval using micro catheter6)Extraction with Bioptome
Finally, we achieved TIMI III flow and patient is completely asymptomatic and we plan a repeat coronary angiography for the patient after 6 months.