
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-033
Coronary Artery Fistula Post Septic Coronary Emboli
By Chanikarn Kanaderm
Presenter
Chanikarn Kanaderm
Authors
Chanikarn Kanaderm1
Affiliation
Central Chest Institute of Thailand, Thailand1,
View Study Report
TCTAP C-033
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Coronary Artery Fistula Post Septic Coronary Emboli
Chanikarn Kanaderm1
Central Chest Institute of Thailand, Thailand1,
Clinical Information
Patient initials or Identifier Number
Supaporn
Relevant Clinical History and Physical Exam
•45years old female
•Underlying disease : None
•CAD risk : None
•Present with prolong fever for 1 month and dyspnea and chest pain for
1hour before visit hospital
•Diagnosed with Inferior wall STEMI, acute MR with heart failure
•Primary PCI to dRCA andPL was perform with clot aspiration and urgency
MVR was done
•At Follow up physical exam show fainting continuous murmur
Relevant Test Results Prior to Catheterization
•First visit
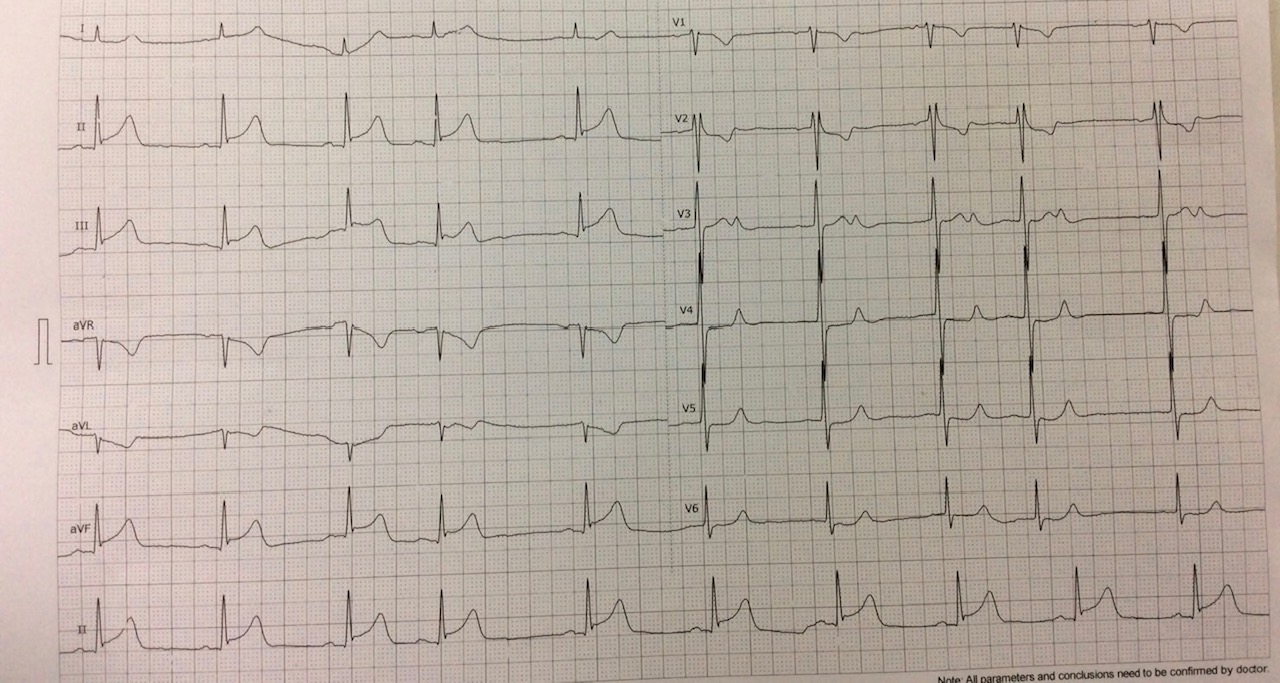
•ECG – ST elevation in lead II,III,aVF ST depress in lead I,aVL
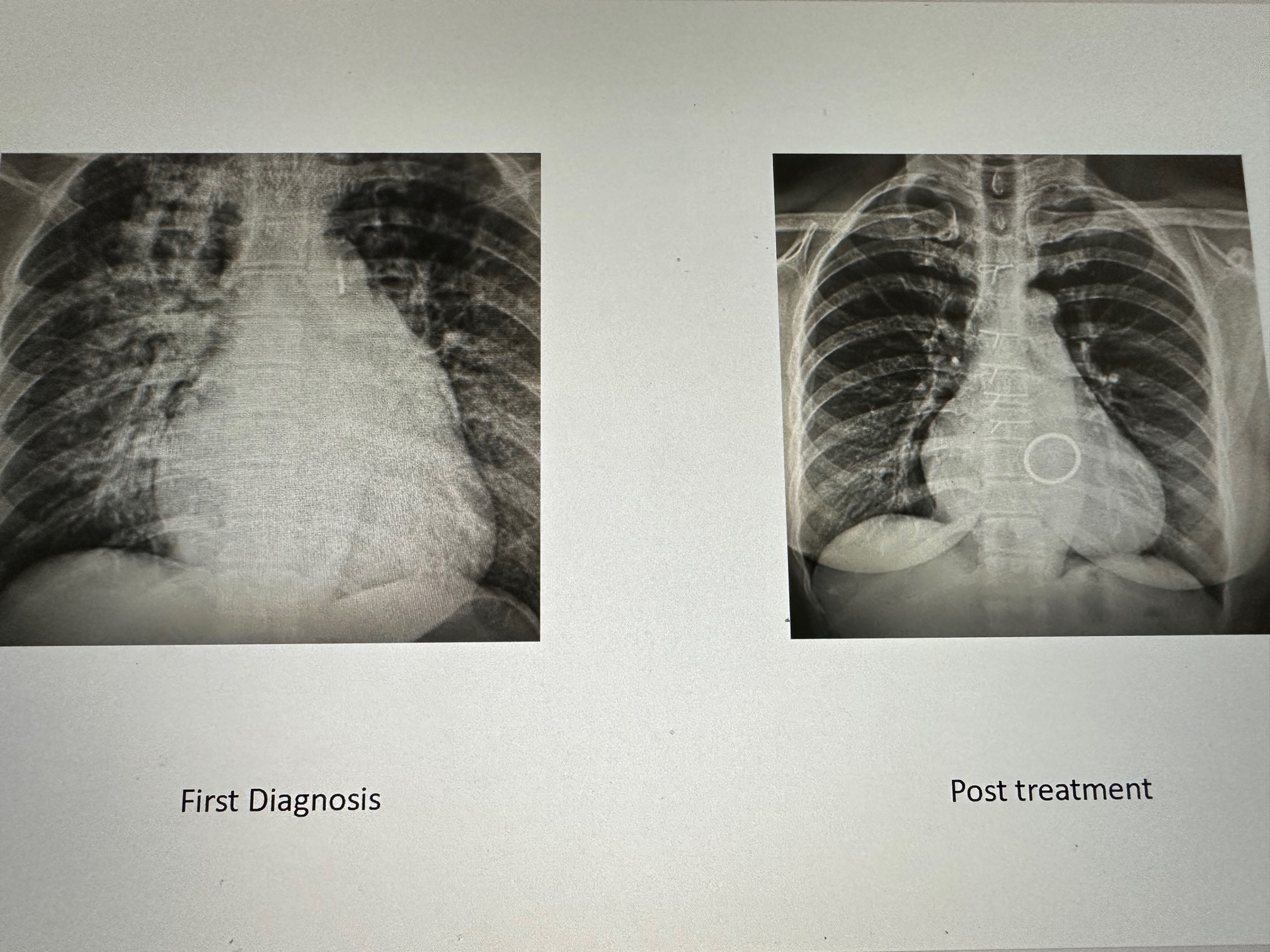
•CXR –Marked cardiomegaly and pulmonary edema
•Echocardiography –Severe MR suspectedPML rupture with vegetation
Relevant Catheterization Findings
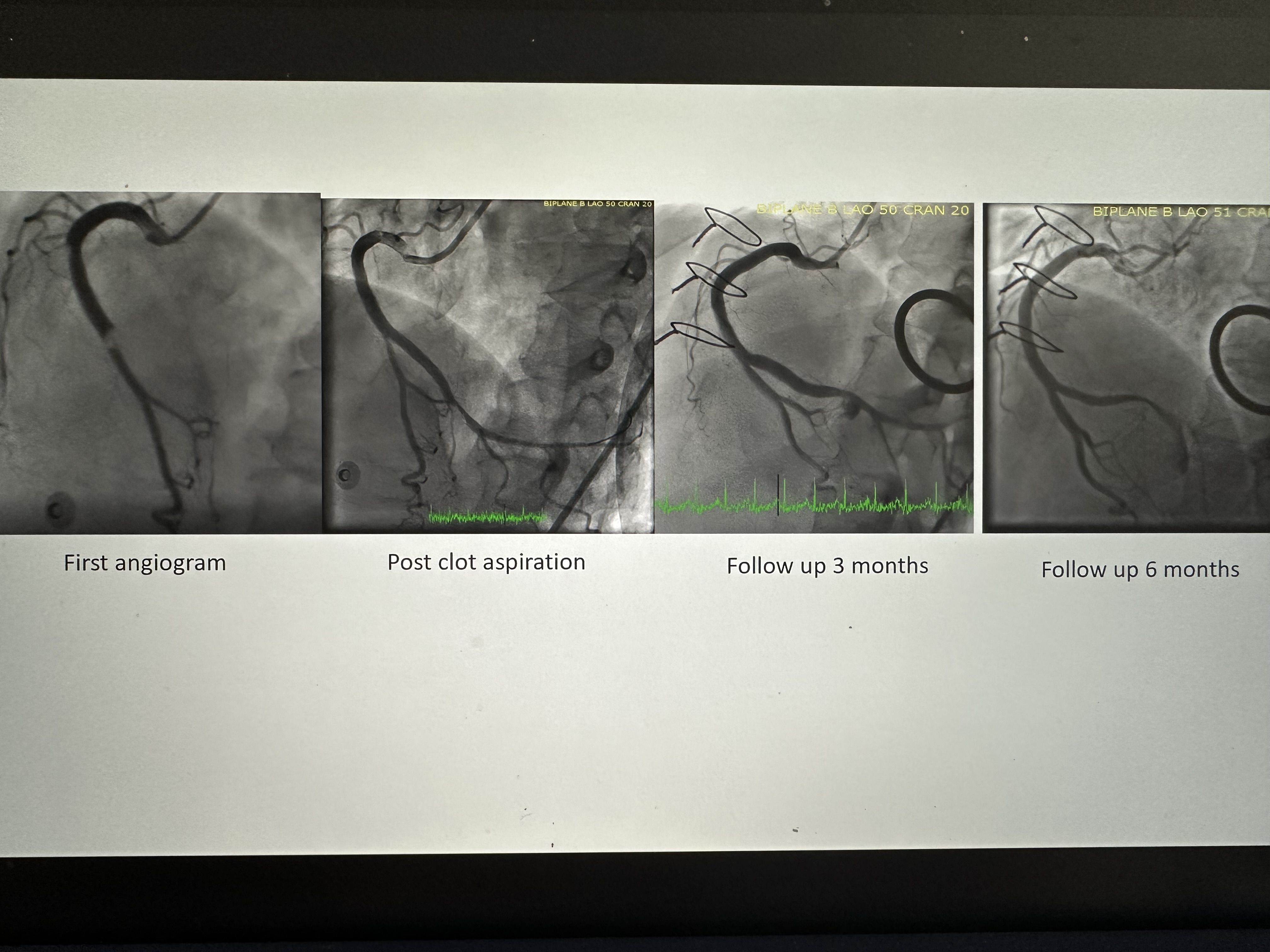
•First coronary angiogram
•LCA -> Normal coronary artery
•RCA-> Total occlude at PL os
•Post primary PCI -> TIMI flow 3 , Mild stenosis at mid PL
•Second coronary angiogram
•RCA -> Aneurysm at PL
•Third coronary angiogram
•RCA-> Coronary AV fistula
Interventional Management
Procedural Step
Using Guiding catheter : JR 3.5/6 Fr. Successful crossing Sion wire to PL . IVUS with Opticross imaging catheter to PL and auto pullback , we measure PL proximal, distal reference and length of Coronary AV fistula . Base on IVUS result ,We plan to use stent graft size 3.0/20 mm. Predilatation and contrast injection balloon occlusion with SC balloon 3.0/15 mm at PL coronary AV fistula site, Stent graft 3.0/20 mm was implant to Coronary AV fistula . Post dilatation with NC 3.0/18 mm. The coronary angiogram show optimal result. Coronary AV fistula was successful occluded with stent graft.
 Image-4.avi
Image-4.avi
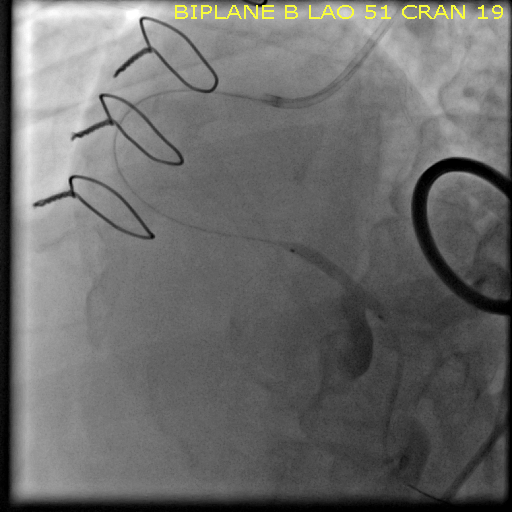
Image-36.avi
Case Summary
- Systemic embolism occurs in patients with Infective endocarditis , including the coronary arteries.-Septic emboli are more frequent with mitral valve infection than with aortic valve infection.-Rare complication after septic emboli in coronary artery is coronary AV fistula.-Coronary AV fistula treated successfully by coronary stent graft deployment.