
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-200
An Interesting Complex Coronary / Valvular / Electrophysiological Intervention.
By Nithesh Kumar, Thoddi Ramamurthy Muralidharan, S Sadhanandham, Nagendra Boopathy Senguttuvan, Manokar Panchanatham, Ramesh Sankaran, Vinod Kumar Balakrishnan
Presenter
Nithesh Kumar
Authors
Nithesh Kumar1, Thoddi Ramamurthy Muralidharan1, S Sadhanandham1, Nagendra Boopathy Senguttuvan1, Manokar Panchanatham1, Ramesh Sankaran1, Vinod Kumar Balakrishnan1
Affiliation
Sri Ramachandra Institute of Higher Education and Research, India1,
View Study Report
TCTAP C-200
STRUCTURAL HEART DISEASE - Valvular Intervention: Aortic
An Interesting Complex Coronary / Valvular / Electrophysiological Intervention.
Nithesh Kumar1, Thoddi Ramamurthy Muralidharan1, S Sadhanandham1, Nagendra Boopathy Senguttuvan1, Manokar Panchanatham1, Ramesh Sankaran1, Vinod Kumar Balakrishnan1
Sri Ramachandra Institute of Higher Education and Research, India1,
Clinical Information
Patient initials or Identifier Number
813849
Relevant Clinical History and Physical Exam
74 year gentle man, known diabetic presented with history of dyspnoea on exertion and easy fatigability for the past 1 month. His general examination was unremarkable, Vitals were stable, Systemic examination revealed a Grade IV Ejection systolic murmur in the aortic area, radiating to the carotids. ECG showed LBBB with left axis deviation with normal PR interval.
Relevant Test Results Prior to Catheterization
Transthoracic Echocardiogram done showed thickened and bicuspid aortic valve with restricted mobility with a valve area of 0.5cm2 (AVA indexed 0.3cm2) by continuity equation. Gradient across aortic valve being mean - 34mmhg, Peak - 68mmhg with global hypokinesia of LV and Severe LV dysfunction (Ejection fraction of 30%).
Relevant Catheterization Findings
Coronary angiogram done showed Mid RCA calcified single vessel disease.

Interventional Management
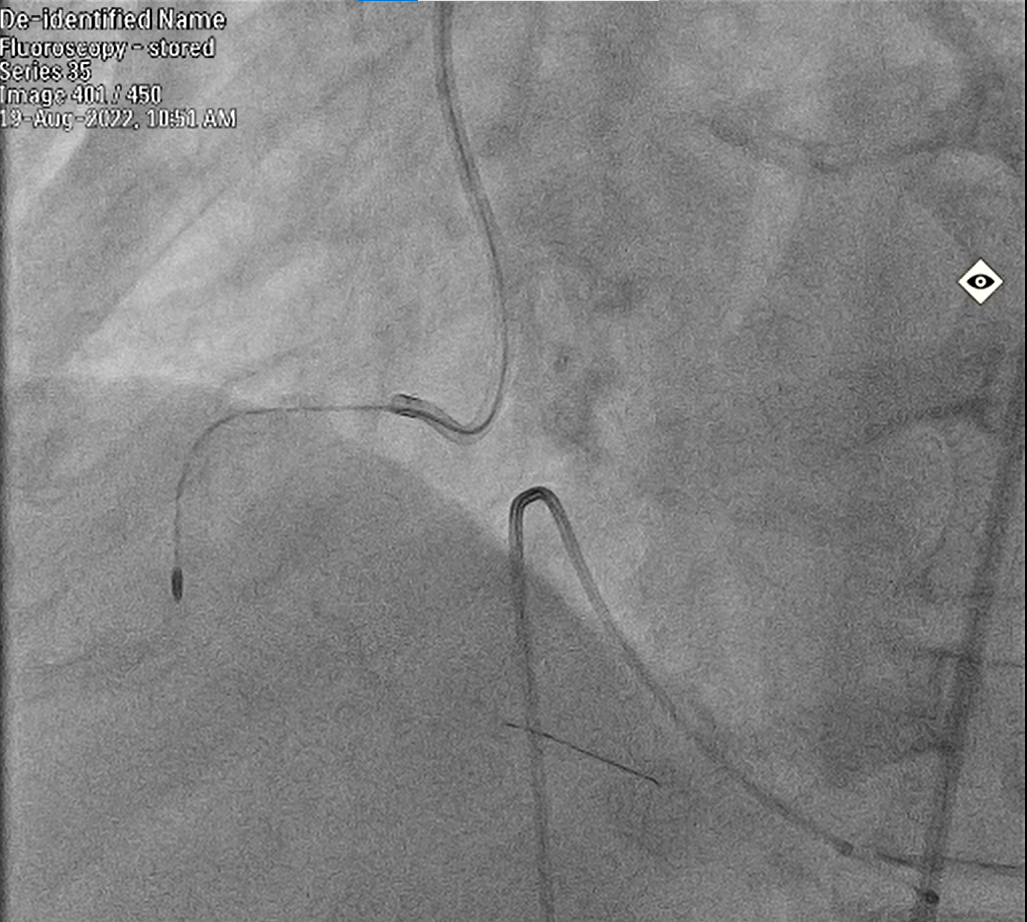
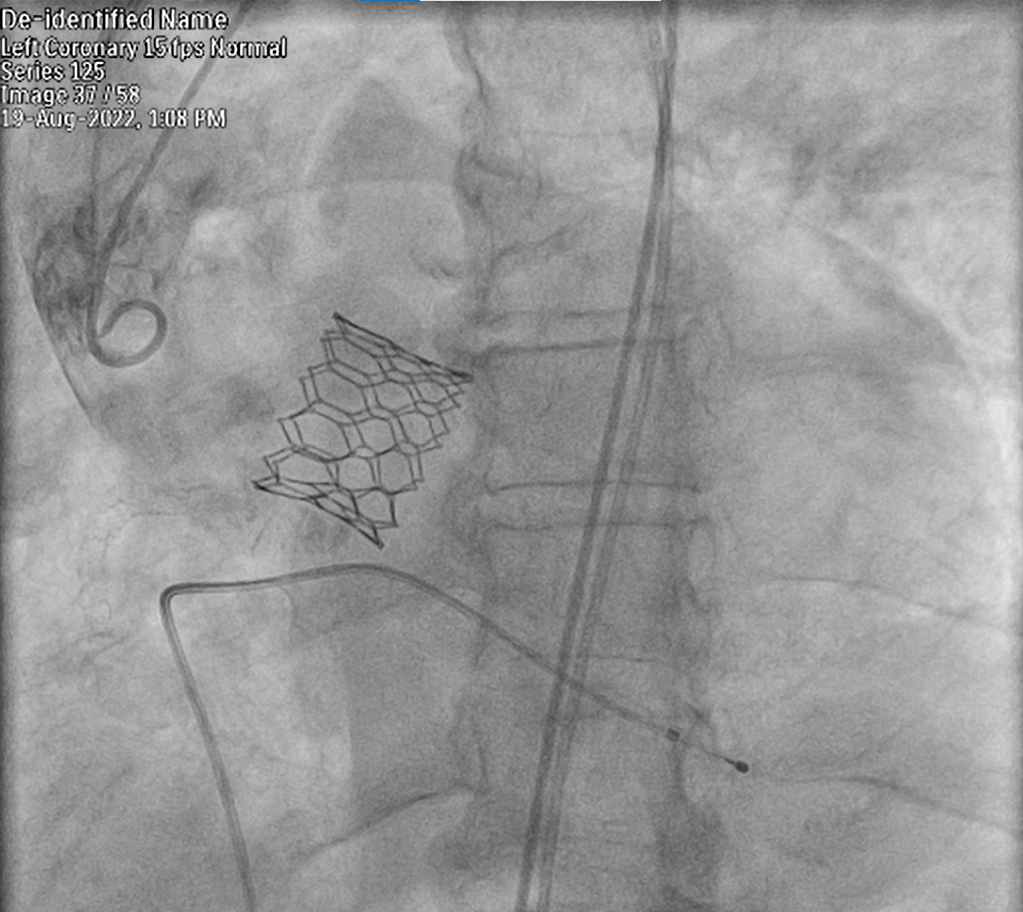
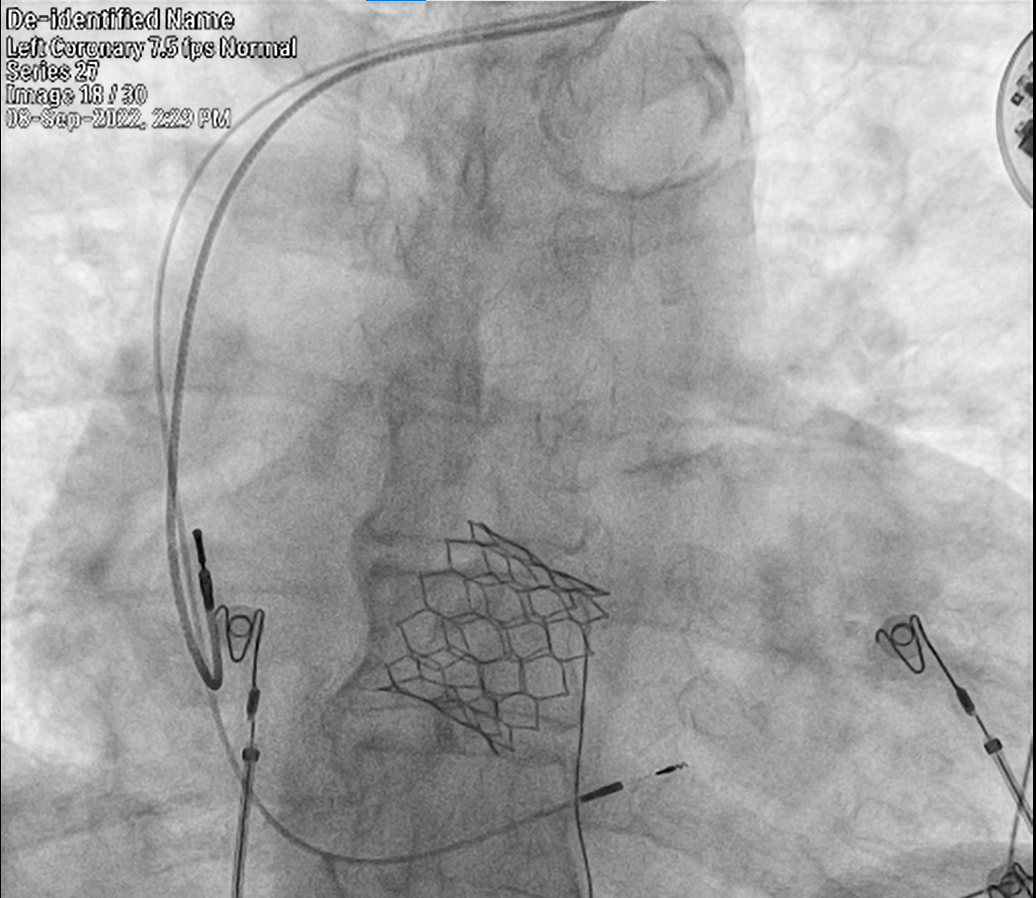
Procedural Step
After adequate preparation, Through left femoral venous approach temporary pacemaker was placed in RV for backup and through left femoral arterial approach 7F long sheath was placed. AR1 guide catheter was used and RCA was selectively engaged. Lesion was crossed with grand slam wire Using guide liner and microcatheter support. IVUS done showed 270-degree calcium arc and a calcific nodule. Grand slam wire was then exchanged for ROTA floppy wire. Rotabalation was done using 1.5mm burr. Further bed preparation was done using 2.75 NC balloon, followed by 3.5mm IVL balloon was crossed and 80 pulses were delivered across the lesion. Using 4.0 X 28mm SYNERGY DES, successfully proximal to mid RCA was stented. Post dilatation was done using 3.5mm OPN NC balloon, followed by 3.75mm OPN balloon. Final IVUS showed good stent expansion. Patient was then proceeded for TAVR. Using right femoral arterial approach 2 perclose devices were deployed, 14F python sheath was placed in the right femoral artery. AL1 and 0.035 straight tip wire were used to cross the aortic valve. Balloon valvotomy was done using 23mm mammoth balloon. 30.5mm(minus 1) MYVAL was deployed after adequate positioning using rapid pacing protocol technique. Transthoracic echo done showed mean gradient across valve of 3mmhg. LV angiogram showed no aortic regurgitation / leaks. Delivery system was removed , perclose devices were deployed, haemostasis achieved and patient was shifted to ICU. Patient after 2 weeks was found to have LBBB with 1st degree AV block, Considering risk of high degree AV block, patient was planned for left bundle area pacing ( Physiological pacing ). Under strict aseptic precautions, Dual access was obtained through left subclavian approach. Infraclavicular pocket was created. RV lead was placed in the left bundle area an lead was screwed. RA lead was introduced through same left subclavian access, placed at RA appendage and screwed. Both the leads were connected to Medtronic pulse generator, parameters were found to be optimal. Pulse generator was kept in the infraclavicular pocket and pocket was sutured in layers. Patient was hemodynamically stable throughout and after the procedure, shifted to ward and subsequently discharged uneventfully.
 TAVI.png
TAVI.png
Case Summary
This case is presented for its complex coronary, valvular and Electrophysiological interventions. Due to the advancement in the field of interventional cardiology, This patient benefitted with improvement in his quality of life. He is on regular follow-up for the past 3 months now, His Aortic valve gradients are low, Ejection fraction / LV systolic function improved, doing well without any complications.