
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-048
Upfront Culotte Technique in a Short Left Main Medina 0-1-1 Lesion That Had Large Calcified Nodule at Ostial Left Circumflex
By Osit Bambat
Presenter
Osit Bambat
Authors
Osit Bambat1
Affiliation
Chiangrai Prachanukroh Hospital, Thailand1,
View Study Report
TCTAP C-048
CORONARY - Bifurcation/Left Main Diseases and Intervention
Upfront Culotte Technique in a Short Left Main Medina 0-1-1 Lesion That Had Large Calcified Nodule at Ostial Left Circumflex
Osit Bambat1
Chiangrai Prachanukroh Hospital, Thailand1,
Clinical Information
Patient initials or Identifier Number
JS
Relevant Clinical History and Physical Exam
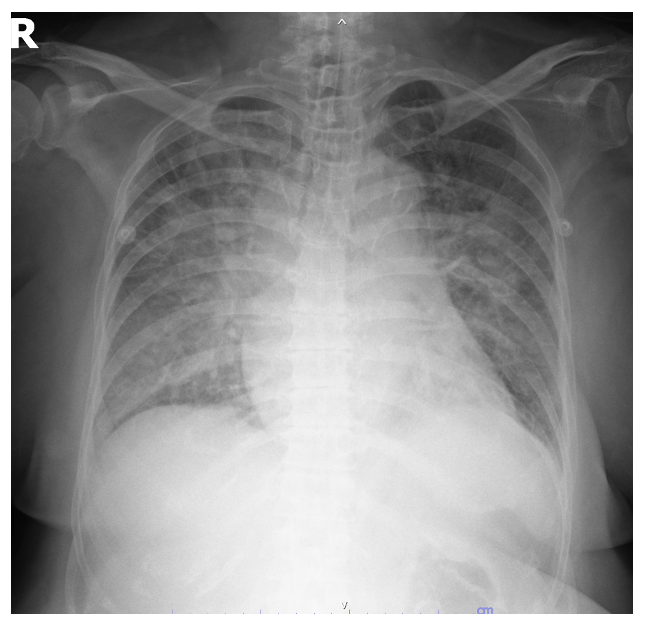
A 65 years old male, with underlying hypertension and gout, who had smoked 20 pack-years and quit smoking for 2 years. He presented at the other provincial hospital 1 month ago with very high risk NSTEMI from heart failure (GRACE score 152) and was referred to our hospital for scheduled CAG.
Relevant Test Results Prior to Catheterization
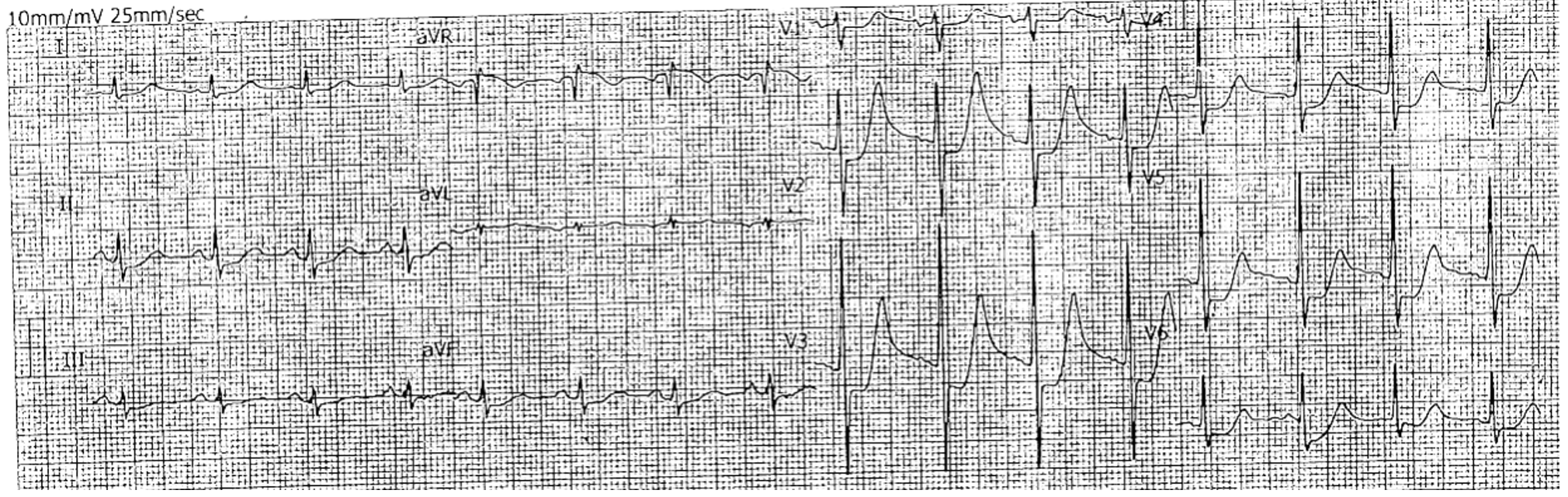
ECG during NSTEMI admission showed normal sinus rhythm, diffuse horizontal ST depression with ST elevation in aVR lead. Hs troponin I was rising from 4312 to 5105 ng/L. He had normal kidney function and no anemia. Echocardiogram showed normal LV systolic function without regional wall motion abnormality.
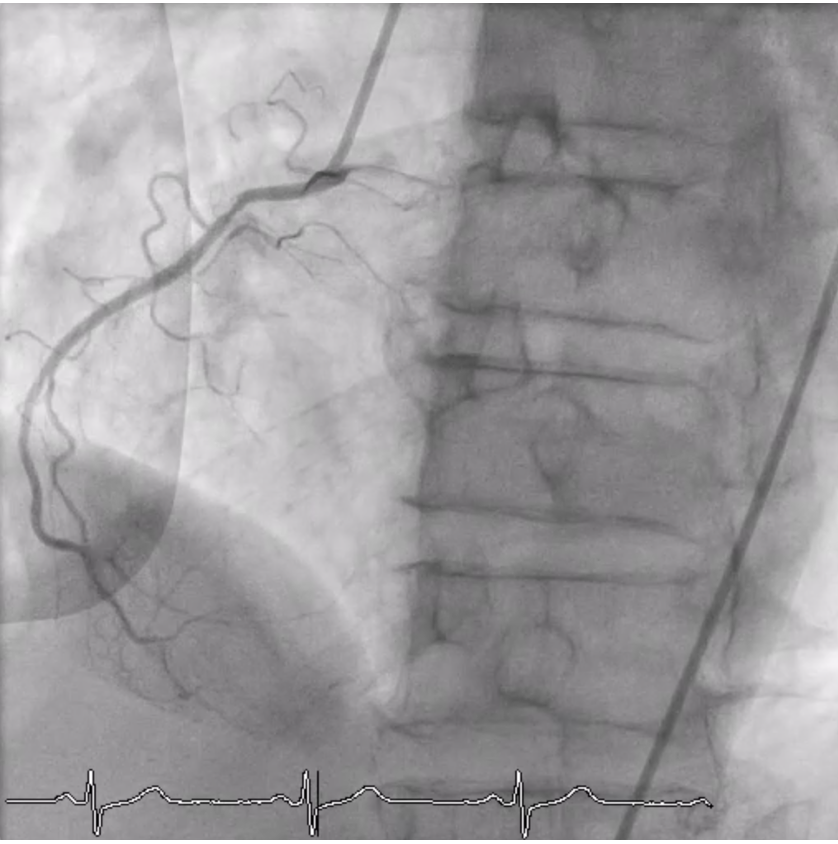
Relevant Catheterization Findings
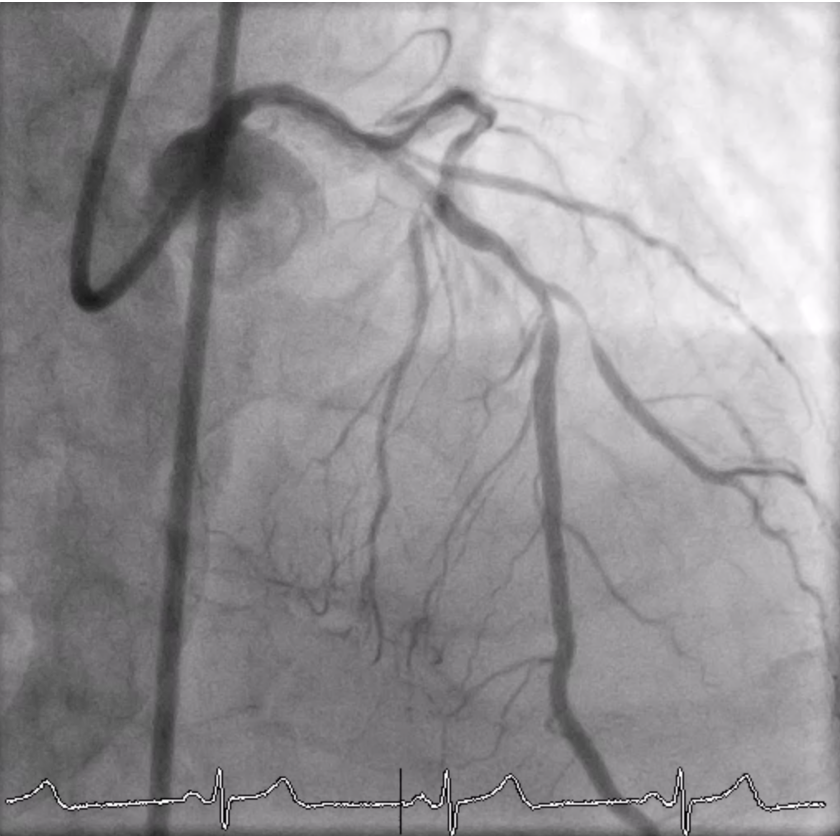
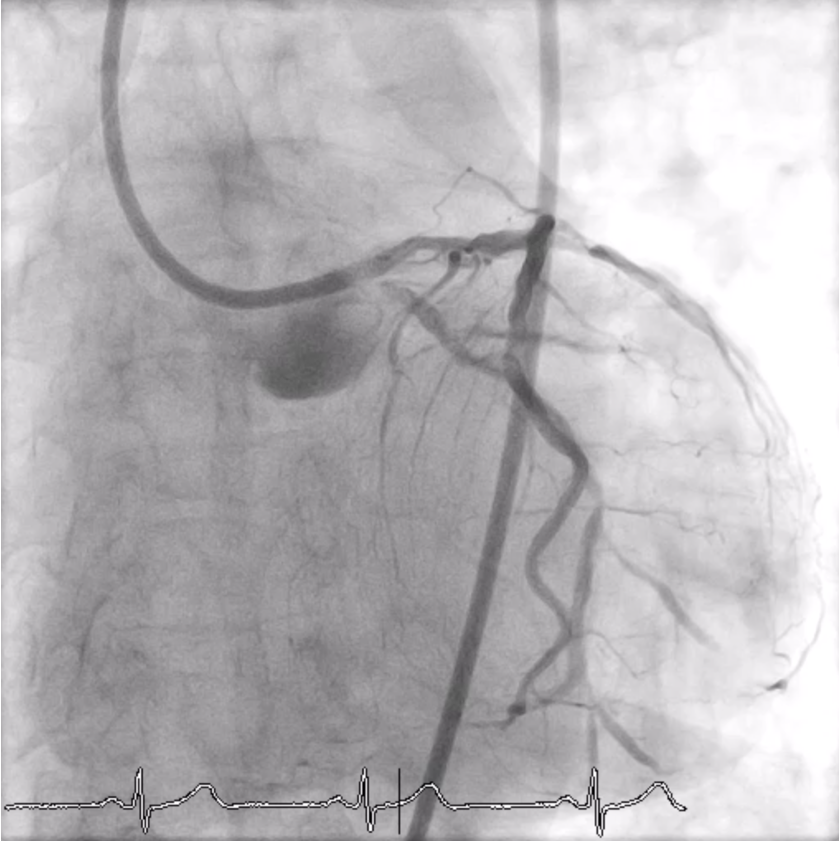
CAG showed left dominant, short healthy LM, triple vessel disease that had severe stenosis at proximal LAD and large calcified nodule at ostial LCX which caused medina 0-1-1. Patient refused the CABG. Staged PCI at LAD & LCX was appointed by using upfront Culotte technique.
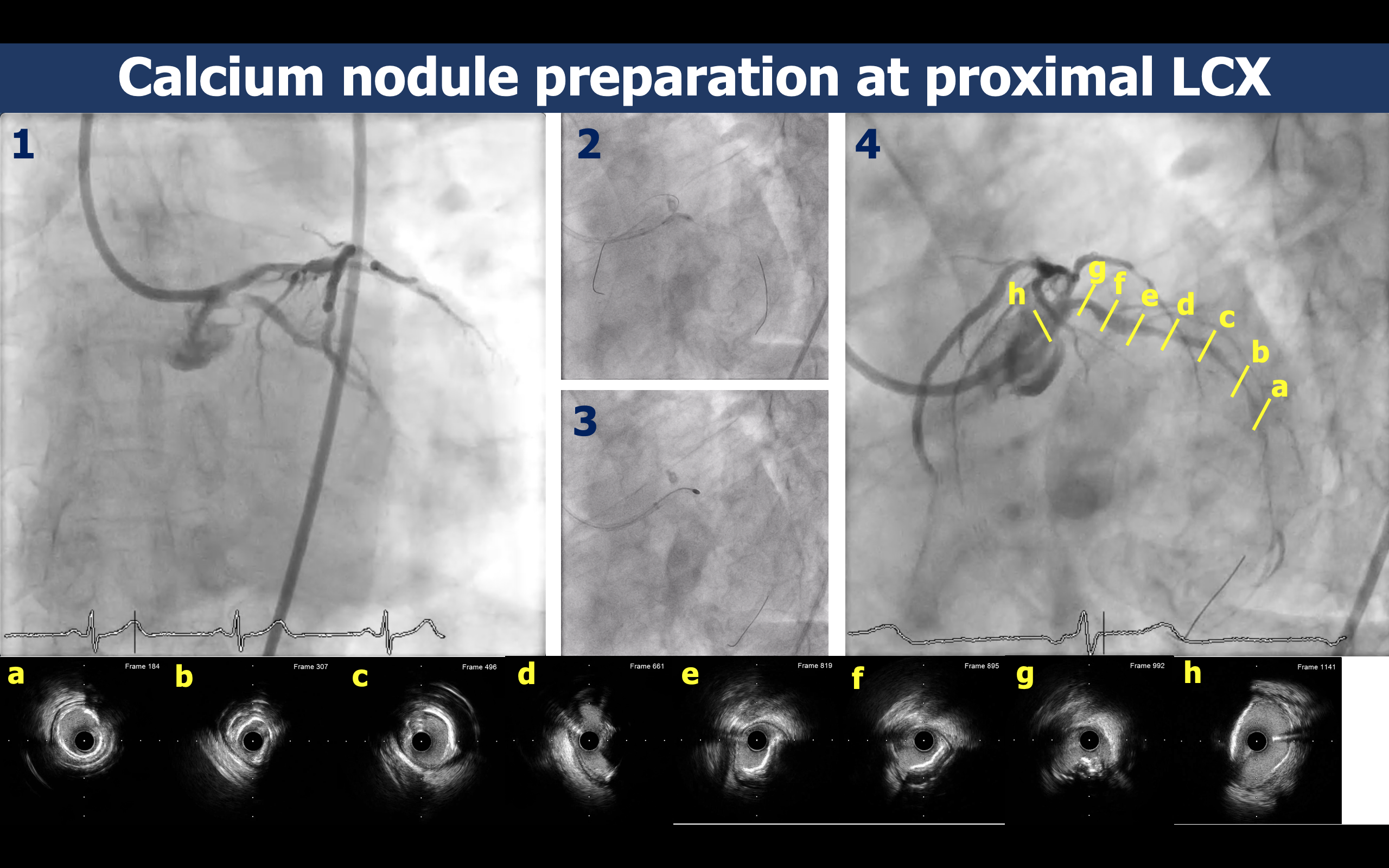
Interventional Management
Procedural Step
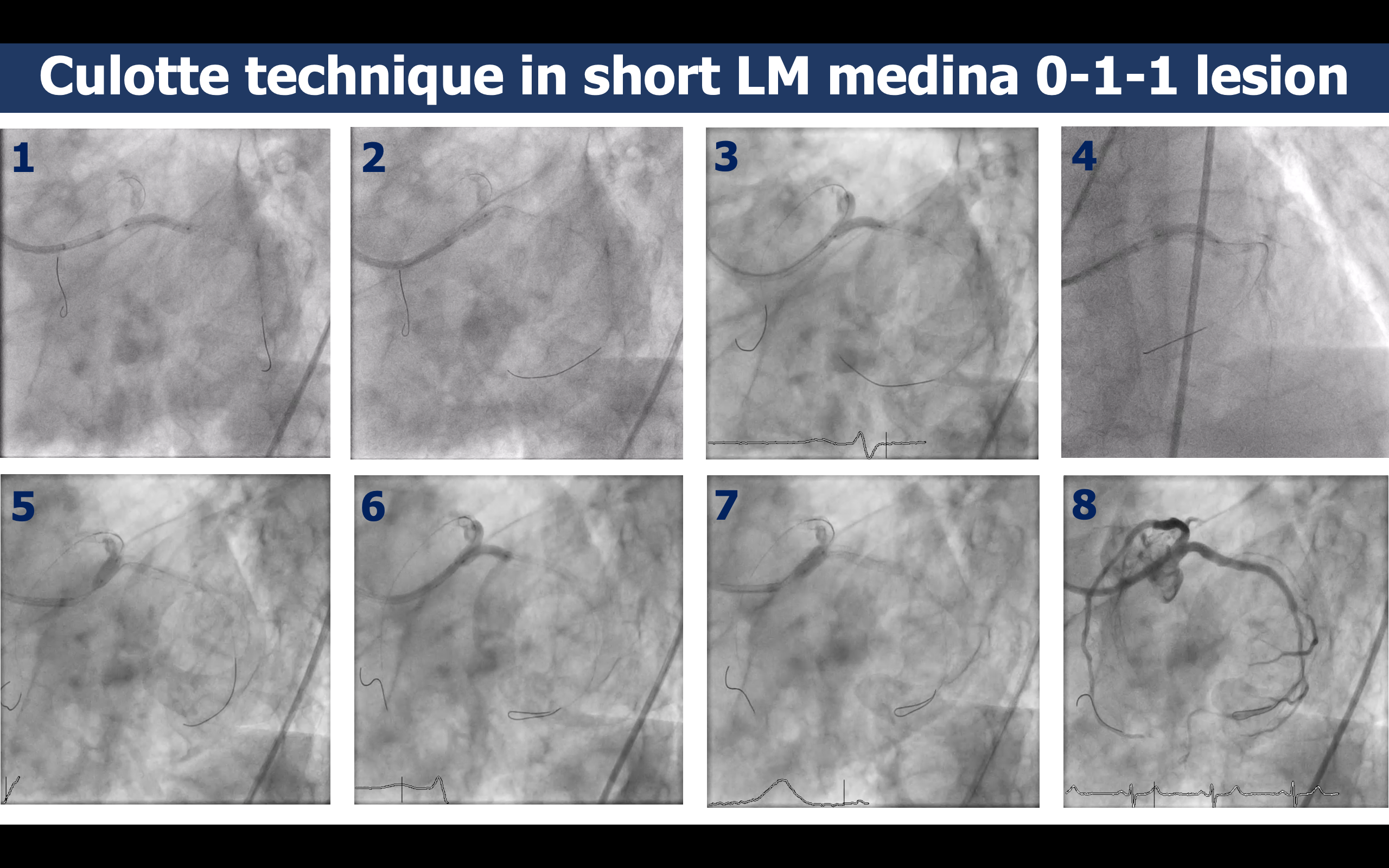
RFA access with EBU 3.5 7Fr was used. IVUS can’t pass ostial LCX then SC balloon 2.5x15 mm was used for predilatation. IVUS showed 270 degree superficial calcification at mid LCX and large calcified nodule at ostial LCX. Rotational atherectomy 1.75 burr on Rota wire extra support was used to debulk the calcified nodule and make the stent fully expand. Culotte technique was chose in this short LM medina 0-1-1 lesion because 1) both LAD and LCX had similar size, 2) angle between LAD and LCX was less than 90 degree, 3) ostial LCX had less stent strut after the MB stent was placed than can easily to rewire and 4) calcified nodule lesion and the carina had 100% covered by the stent.After predilatation along LCX with NC balloon 3.0x20 mm, 3 DESs were deployed from LM to mid LCX by using guiding extension to enhance stent delivery past the calcified nodule. First POT, rewire, kissing was done and a fourth DES was deployed from LM to proximal LAD. Second time of POT, rewire, kissing was done at LM bifurcation with final POT for elliptical correction at LM stents. Another 2 DESs were placed from proximal to mid LAD.
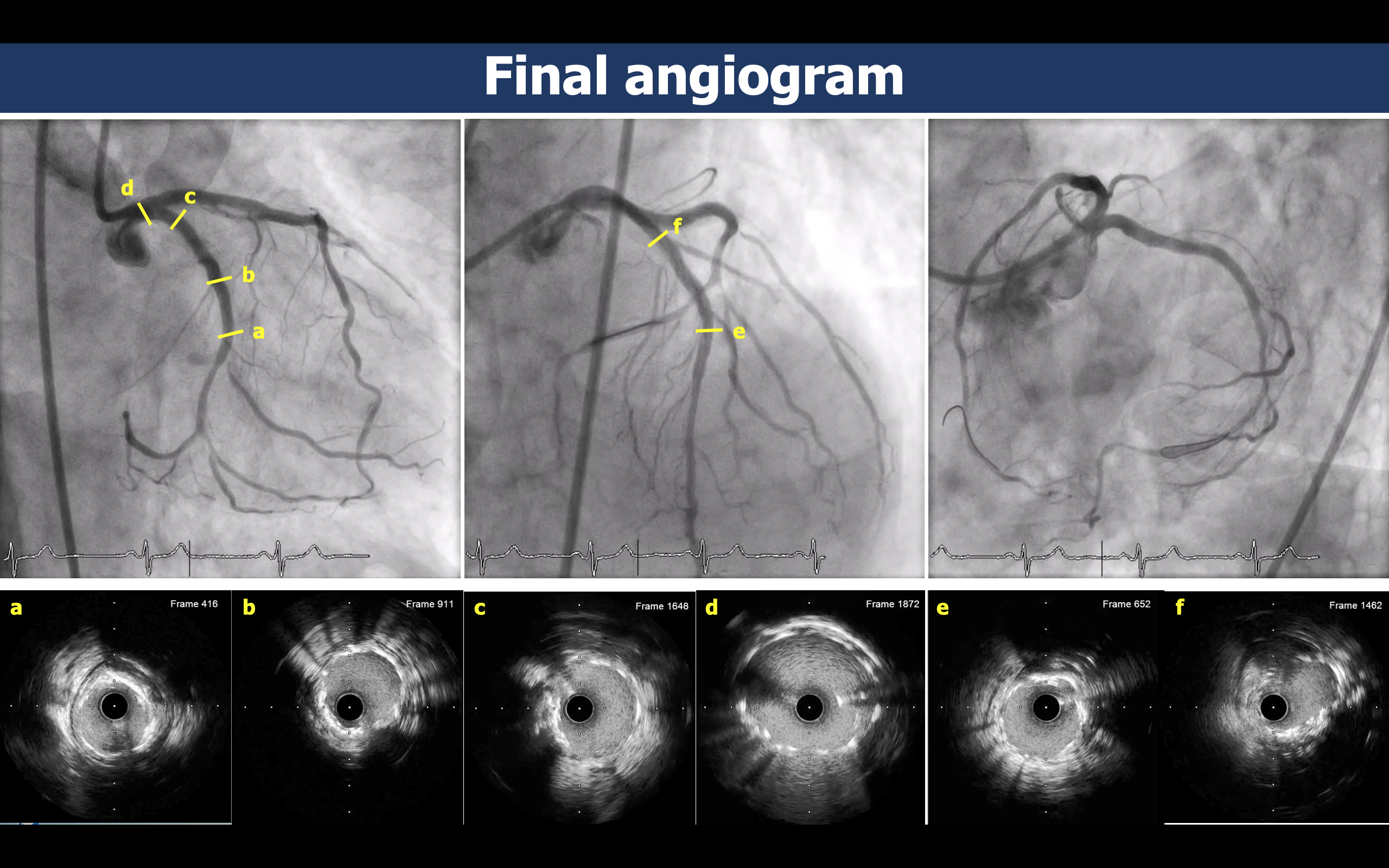
Case Summary
Upfront Culotte technique may be feasible in the short LM medina 0-1-1 lesion with calcified nodule at ostial LCX.Rotational atherectomy was used to debulk the calcified nodule and make the stent fully expand at the calcified nodule lesion.